This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
saline (NS) solutions are both isotonic crystalloids widely used for intravenous fluid resuscitation across many contexts and disease states ( Myburgh 2013 ). Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. Lactated Ringer (LR) and 0.9% To assess the clinical impact and relevance of these concerns, Alwang et al.
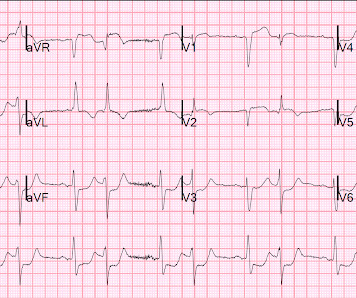
A prehospital ECG was similar to the first ED ECG, which is shown below. Here is her initial ED 12-lead ECG: There is atrial fibrillation with a rate of approximately 114. It is most commonly due to demand ischemia, not due to ACS! If it were ACS, what reperfusion options were available? 911 was called. What happened?
Causes: ACS, arrhythmia, valvular dysfunction, infection, nonadherence to meds, myocarditis, volume overload. ACEP level C recommendation that while there is no specific timing for diuretic therapy, physicians can consider earlier administration of diuretics in ED patients with HF (ACEP). J Am Coll Cardiol 2013; 62(16):e147–239.
This is really good Prehospital, ED, and Cardiolog. Fever, tachycardia, hypotension, hypoxia and "SVT" A woman in her 40s with palpitations and chest pre. Flecainide toxicity 4/21/21 2597782 This case was flagged as a false positive cath lab. A man in his 60s with diaphoresis, vomiting, and i.
The syphilis and trichomonas tests come back negative in the ED, but his rapid HIV test is positive. How should clinicians approach the diagnosis and management of HIV in the ED? 11 These cardiovascular complications have further increased ED visits by HIV-positive patients by three times compared to individuals without HIV.
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
Ed Burns (from Life in the Fast Lane) sent me this. See what happens when one fails to diagnose STEMI. Serial ECG recordings are essential: paramedic mak. Are These Wellens' Waves?? .
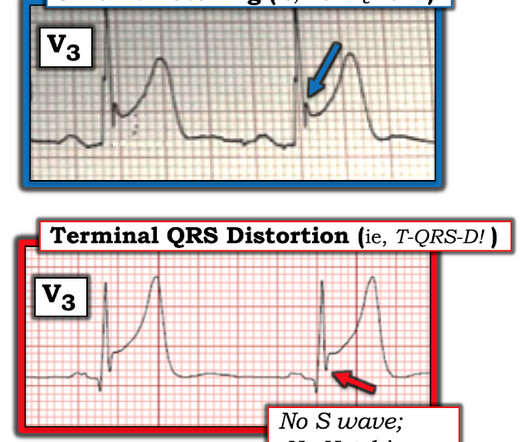
Emergency (ED placement) Transvenous Pacer appears. Back to basics: what is this rhythm? What are your. 30 yo woman with trapezius pain. HEART Pathway =. Good case for showing a flutter and LBBB, Good cas. What is this rhythm? Back to basics. Is there Terminal QRS Distortion? What is so unusual about this inferior OMI (which.
A 20-something woman with Chest Pain Eric Abrams case A woman in her 50s with dyspnea and bradycardia Where is the focus of this tachycardia? Ventricular Fibrillation, ROSC after perfusion res.
Dysnpea and Elevated troponin Takotsubo that looks like LVA Huge Precordial ST Elevation in an ED Patient Tachycardia, hyperthyroid, and ST elevation. Is this just right bundle branch block? Besides the Nonspecific T-wave Inversion in aVL, W.
Chest pain resolved, and a "Normal" ED ECG 2 cases of false pos STE aVL What will you do for this patient transferred to y. 30-something male with confusion, weakness, headac. A Patient with Respiratory Failure and a Computer. Cardiac arrest with STEMI pattern: no acute corona. How accurate are the Monitor leads for ST Elevation?
A 5-year-old female presented to the emergency department (ED) with a one-year history of gradually increasing anterior neck swelling. She was discharged from the ED on levothyroxine 25 mcg daily with endocrinology outpatient follow-up. 2013 Mar;34(3):115-24; quiz 125. The patient had no significant past medical history.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
mL/kg/hr for 2 consecutive hours OR Decrease in serum lactate by more than 10% from initial level Primary outcome – Early norepinephrine group vs. the control group demonstrated higher rates of shock control at 6 hours: 76.1% vs 48.4% (OR 3.4, vs 48.4% (OR 3.4,
Abdominal pain is a common ED presentation and one of the top differential for RLQ pain is Acute Appendicitis. References Meltzer AC, Baumann BM, Chen EH, Shofer FS, Mills AM. 2013 Aug 1;62(2):126-31. Early in the course, examination findings are often subtle and bloods may not show a raised WCC or CRP.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. After all, there is no S wave in lead V3.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Chou’s Electrocardiography in Clinical Practice, 6th ed. Goldberger’s Clinical Electrocardiography: A Simplified Approach, 9th ed. Annals of Noninvasive Electrocardiology, 18 (1), 21-28.
She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Here is an article I wrote: Updates on the ECG in ACS. Was this: 1) ACS with ischemia and spontaneous reperfusion? Current Emergency and Hospital Medicine Reports (2013) 1:4352. If you want to understand aVR, read this.] References : 1.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
This was formerly an indication for cath lab activation, but was abandoned in the 2013 guidelines because of poor specificity. The best study was an ED study that showed that about 7% of patients with chest pain and new LBBB in the ED were diagnosed with acute MI. This patient presented to the ED with complete LBBB.
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. Although this is considered a "STEMI equivalent" and the ACC/AHA guidelines even approve of thrombolytics for ACS with this ECG, the usual criteria used to alert the cath lab team of an inbound Code STEMI are not met by this ECG.
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Card 1999; 34:748-753. O'Gara et al. Circulation. mm in ≥ 1 posterior lead and has few false positives. (6)
Posterior STEMI" may not even technically exist according to the current (2013) ACC/AHA STEMI guidelines, as it is not described as a "STEMI equivalent" and the only relevant statement in the guidelines is: "In addition, ST depression in 2 precordial leads (V1-V4) may indicate transmural posterior injury."
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk. To date, ketamine has been the agent of choice (12).
Pre-school wheezers remain a poorly understood cohort of children despite seeing them every day in paediatric EDs. However, there was no difference in LOS (83 minutes for placebo vs 79 minutes for prednisolone) in participants who were discharged straight from the ED ( 32% ). Reattendance to GP/ED was more important.
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. 7) The 2013 ACC/AHA STEMI guidelines consider this a “STEMI equivalent,” where thrombolytic therapy is not contraindicated (Evidence level B, no specific class of recommendation).(16) TIMI 0/1 flow).(61,62)
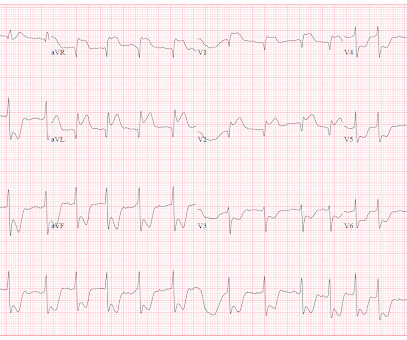
She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. BP gradually rose. This ECG is diagnostic of diffuse subendocardial ischemia.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
As the only respiratory therapist in the ED has been paged and is starting BiPAP for this patient, an overhead call for two incoming trauma alerts from a multivehicle collision sounds. Because the RT responsible for drawing arterial blood gases is busy caring for these patients, ABGs will be delayed.
These are send-out labs with turn-around times that make them unlikely to affect the ED course. This prevents ongoing exposure to the patient and ED staff. In: Mattu A and Swadron S, ed. Published 2013 Dec 9. Published 2013 Dec 9. 3 However, may be helpful in diagnosing the chronic toxicity forms. CorePendium.
Arch Dis Child Fetal Neonatal Ed. Arch Dis Child Fetal Neonatal Ed. 2023 May;182(5):2013-2026 QuantiFERON-TB Gold Plus Performance in Children: A Narrative Review. De Alwis AC, et al. Hypertension in Wilms tumor. Hsiao W, et al. Pediatr Nephrol. 2023 May 13. Mullaly R, et al. 2023 May 12:fetalneonatal-2022-324935.
An 8-year old male with a history of sickle cell anemia presents to the ED for evaluation of fever for 2 days and “feeling like I can’t get a full breath”. 768: Epidemiology of Hospital Based ED Visits due to Sickle Cell Crisis and Acute Chest Syndrome in Kids. Critical Care Medicine 41(12):p A191, December 2013. C or 100.4
F, HR 48, RR 28, BP 104/62, SPO2 88% on non-rebreather mask The patient’s friend who brought her to the ED tells you the patient made suicidal statements earlier in the day and was found in her yard shed. These are send-out labs with turn-around times that make them unlikely to affect the ED course or guide treatment. 2013; 6:524.
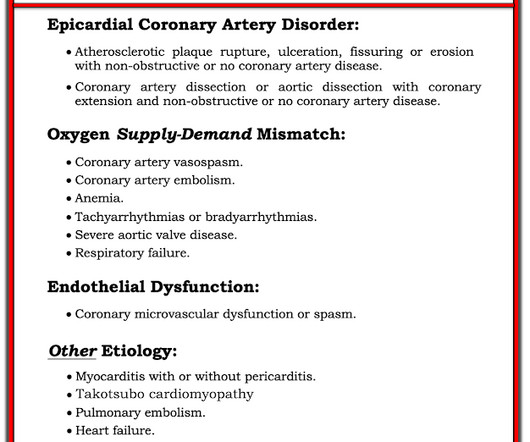
He arrived in the ED and had this ECG recorded: The first high sensitivity troponin I returned undetectable (3 ng/L). The 3 most common causes of ACS ( A cute C oronary S yndrome ) without coronary disease are: i ) Myocarditis ( up to 1/3 of these patients ); ii ) Takotsubo cardiomyopathy; and , iii ) MINOCA.
Patients with suspected ACS should be evaluated with echocardiography. Incidence and Prognosis of Pericarditis After ST-Elevation Myocardial Infarction (from the Acute Coronary Syndrome Israeli Survey 2000 to 2013 Registry Database). Perhaps not all readers of this blog are experienced evaluating echo images. References: [1] Lador, A.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content