This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. We’re expected to routinely give heparin for all these NSTEMI and unstable angina patients with any ischemic changes seen on the ECG, right? And for STEMI too. But should we?
On this month's EM Quick Hits: Christina Shenvi on ACS in older people, Nour Khatib on rural NRP, Jess McLaren on how not to get fooled by ECG computer interpretation, Brit Long on hemophilia recognition and workup, Maria Ivankovic on persistent and intractable hiccups from EM Cases Summit 2021.
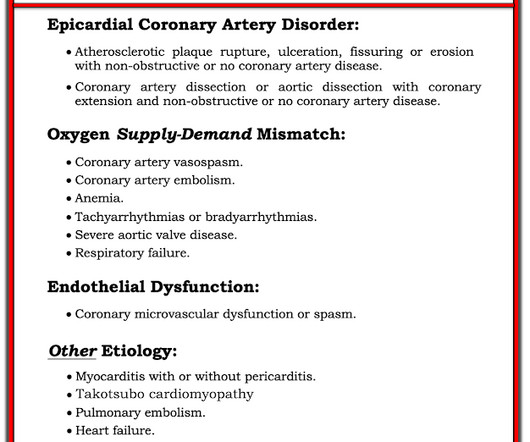
Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). Access the links provided for a detailed review of varying ECG patterns when ACS breaches the typical subendocardial ischemia pattern. Type I ischemia. Type II ischemia.
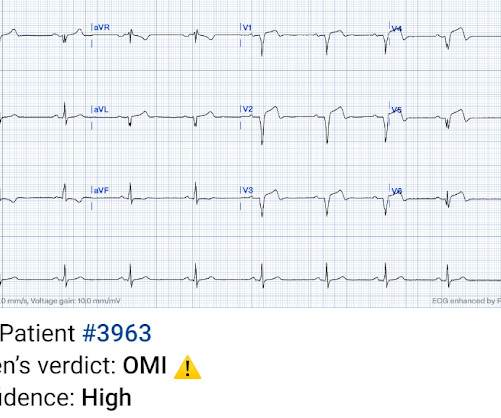
By Smith, peer-reviewed by Interventional Cardiologist Emre Aslanger Submitted by anonymous A 53 y.o. male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. The pain radiated to both shoulders. He arrived to the ED at around 6:45am, and stated the pain has persisted.
EDACS is broader—captures symptoms suspicious for ACS, not just chest pain, and performs well in low-risk patients. Clinical Bottom Line Both HEART and EDACS are best utilized for identifying patients with suspected ACS who are at low risk for MACE. Cardiovascular Read More REBEL Cast Ep114: High Flow O2, Suspected ACS, and Mortality?
What are the most useful historical factors to increase and decrease your pretest probability for ACS? Which cardiac risk factors have predictive value for ACS? In the age of high sensitivity troponins and the HEART pathway, which patients are safe to discharge home from the ED?
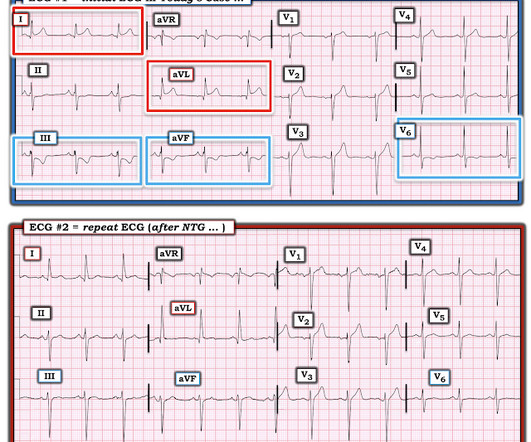
This dynamic change is diagnostic of ACS. Cardiology was consulted and agreed that his history was high risk for ACS and a next-day angiogram was merited. This was also non-diagnostic for OMI, although the dynamic changes are diagnostic of ACS. ECG at time 82 minutes: What do you think?
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” ACS is usually amongst this differential, as cardiovascular disease is a leading cause of morbidity and mortality in this population. The proportion of patients with ACS at the index visit or within 30 days. *
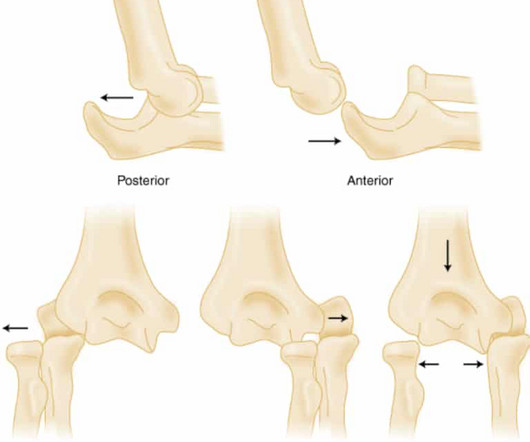
J Bone Joint Surg Br. 2001;83:1173-5. Oakley EA, Ooi KS, Barnett PLJ. A randomized controlled trial of 2 methods of immobilizing torus fractures of the distal forearm. Pediatr Emerg Care. 2008;24:65–70. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117:691–697.
Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. PMID: 28106307 Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. To assess the clinical impact and relevance of these concerns, Alwang et al. performed the retrospective cohort study below ( Alwang 2024 ). JAMA Intern Med. 2024;184(11):1365-1372. Microcirculation.
ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. Then ACS (STEMI) might be primary; this might be cardiogenic shock. One must clearly rule out these processes before jumping on the ACS diagnosis. Are the lungs clear? Is the patient cool and pale?
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." Chest pain or discomfort) What do you think? Here was my response: "Suspicious for inferior posterior OMI.
In this ECG Cases blog we look at 6 patients who presented with cardiorespiratory symptoms, possibly from COVID and illustrate the dangers of anchoring, being hypervigilant for cardiovascular complications, and why testing for COVID in patients being admitted for ACS is important.
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. A bedside echo performed by the emergency physician showed no wall motion abnormality and confirmed LVH.
Then assume there is ACS. Therefore — recognition of DSI on ECG should prompt consideration of 2 Categories of diagnostic entities : Severe Coronary Disease ( due to LMain, proximal LAD, and/or severe 2- or 3-vessel disease ) — which in the right clinical context may indicate ACS ( A cute C oronary S yndrome ).
Big changes are on the horizon for trauma centers participating in the American College of Surgeons (ACS) Trauma Quality Programs (TQP). We’ve been working closely with the ACS to prepare for this transition. The ACS is aware that we are not updating the legacy registry products. What’s changing?
Pain episodes, or vaso-occlusive crises (VOC), are a hallmark of sickle cell disease, often leading to prolonged hospital stays and serious complications like acute chest syndrome (ACS). While small studies suggest that early pain relief can shorten hospitalisation, the evidence remains limited.
Takeaway lessons * If considering ACS in any post-menopausal woman, you should also consider stress cardiomyopathy. Of course, atypical anatomical distributions can also occur in ACS due to distinct anatomy. ACE inhibition). * In general, TCM is a diagnosis of exclusion after ruling out ACS. Find us on Patreon here!
I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. Of interest, he specified that he awoke earlier that morning in his usual state of health, then developed chest discomfort, then developed palpitations.
It is important to note that these findings, if due to atherothrombotic acute coronary syndrome (ACS), are NOT due to occlusion of the left main, as is frequently stated in online postings and in literature. It is most commonly due to demand ischemia, not due to ACS! If it were ACS, what reperfusion options were available?
ACS is dynamic. interesting spontaneous reperfusion case 1413140 prehospital STEMI first ED ECG is here, with 3/10 pain: But this is the same patient just 10 minutes before, with 7/10 pain Isn't it ridiculous to say that the patient has both a STEMI and an NSTEMI? It can't be given one static name. Now the patient has one disease: OMI.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center.
One must remember that acute pulmonary edema is frequently triggered by ACS. In this case, it is reasonable to assume that there is no ACS. Here is the troponin profile: Troponins this high are almost always due to type 1 MI (ACS, plaque rupture) This was a surprise. Severe, life threatening ACS may have no ST Segment shifts.
These have all been small studies, studying very few patients with ACS, and often used final cardiology interpretation rather than patient outcome. Smith : This study had such low risk patients that not a single patient was ultimately diagnosed with ACS. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
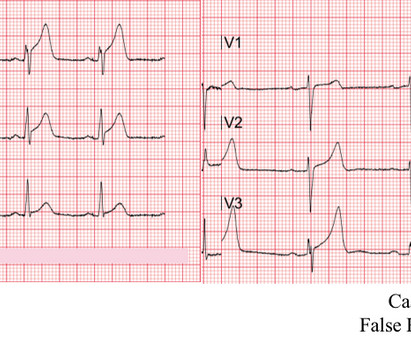
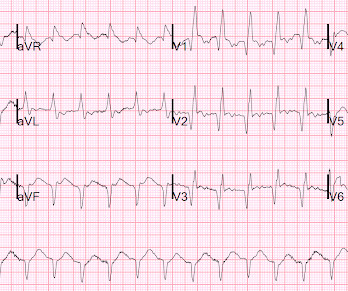
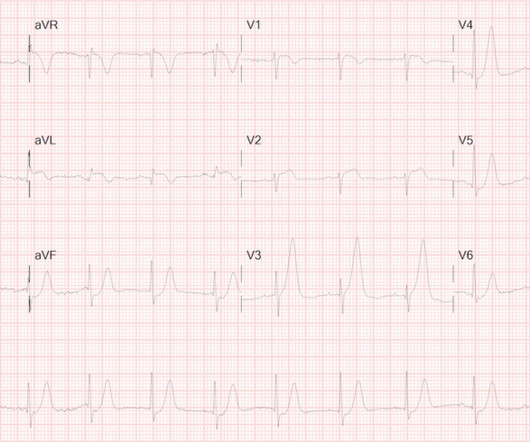
References: Kimbrell J, Kreinbrook J, Poke D, Kalosza B, Geldner J, Shekhar AC, Miele A, Bouthillet T, Vega J. The conversation concludes with a discussion on the transfer of pacing from one device to another and the importance of verifying capture during the process. Check out more from Josh, Judah, and Tom at EMS12LEAD.com. 2024 Mar 15:1-9.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. ECG's are difficult.
” The researchers presented their technology at the 2022 fall meeting of the American Chemical Society (ACS). Via: ACS. . “We already interact with a lot of touch-based electronics, such as smart phones and keyboards, so this sensor could integrate seamlessly into daily life.”
3) ACS with possible additional ischemia from atrial fib with RVR 4) Hemorrhage/dehydration/sepsis/etc., I was fairly certain that this was a type II (demand ischemia) MI and that this patient was not having ACS. He did not have ACS. Not all myocardial infarction is due to ACS 2. He was treated for urosepsis and did well.
The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The patient was a middle-aged female who had acute chest pain of approximately 6 hours duration. The pain was still active at the time of evaluation.
Comment : ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). The ESC states that patients with suspected ACS should go to the cath lab in <2 hours "regardless of ECG or biomarker evidence of MI!!"
If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. The new ESC guidelines has for the first time merged both STEMI and non-STEMI in the same guideline because they are both on the spectrum of ACS.
The bottom line from that episode was that the HEART Pathway appears to have the potential to safely decrease objective cardiac testing, increase early discharge rates and cut median length of stay in low-risk chest pain patients presenting to the ED with suspicion of ACS. If we thought about ACS, we brought them in. AEM June 2022.
DOI: Papudesi BN, Malayala SV, Regina AC. This month in JAAD Case Reports: August 2023: Xylazine and skin necrosis. Journal of the American Academy of Dermatology. 2023 Aug 1;89(2):231. Xylazine toxicity. 2023 [book]. PMID 37603662 Rose L, Kirven R, Tyler K, Chung C, Korman AM. JAAD Case Reports. 2023 Jun 1;36:113-5.
This should prompt immediate investigation into supply-demand mismatching, or ACS. There is bradycardic Atrial Fibrillation with broad ST-depression in most leads and perceptible ST-elevation in aVR. But there’s some peculiar features about this ECG: The unusually short QT The “scooped out” appearance of the ST-segments.
Blood sampled from existing peripheral IV cannulae yields results equivalent to venepuncture: a systematic review [ 10.1177/2054270419894817 ] Second Line 18 G Should we be placing in the AC? Future Show: Upping your IV Game Fluids Get dinged for 4, rectal temps on elderly, etc.
One study found that the best discrimination of stress cardiomyopathy from ACS was possible with the ratio of NT-proBNP/cTnT on the 2nd day. and an accuracy of ∼96% in detecting stress cardiomyopathy as opposed to ACS. NT-proBNP and CTnT in ACS and Takotsubo) Smith : However, this is not of any help with the acute diagnosis!
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data. References: 1.
He was started on ACS therapy and loaded with Plavix. This procedures were done due to prior similar presentations and concern of ACS. This is the most likely caused of his fixed ST elevation and no concern for ACS. Initial ECG showed ST elevation with progression of biphasic T wave concerning for reperfusion injury.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Link to abstract Link to full text 2) Use of Morphine in Non-STE-ACS is independently associated with mortality, at odds ratio of 1.4
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content