This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Many agencies simply default units that are on duty with a general “available” status whenever they are not in some active phase of a specific response. The common impression is that this is an unproductive time embodying only the cost of preparedness. Increasing pressure on limited EMS resources suggests benefits to a more detailed appreciation of the precise nature of any unit or crew in this generic status.
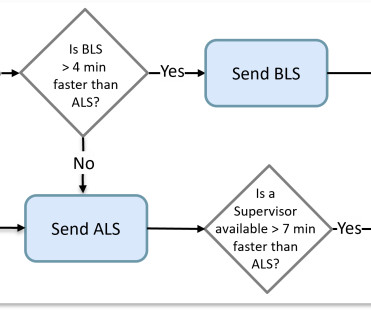
The traditional method for planning EMS responses has always been a static process developed with simplistic rules using arbitrary times as the primary goal. Yet every dispatch decision must be made in real-time from a changing list of possibilities focusing on the potential impact of each option. Matching the rules of your decision logic with the actual process shifts the focus toward system efficiency and effective patient-centric outcomes.
Great OpEd published by AIMHI about how our industry is changing and leading to “EMS On Life Support: The Alarming Gap Between Expectations and Reality.” [link] I have been writing a lot this year that “ a stopwatch is not a valid instrument for summarizing the measure of care that a patient receives. ” What any administrator, or politician, should be concerned with is the quality care they are buying before the simplistic statistics they are generating.
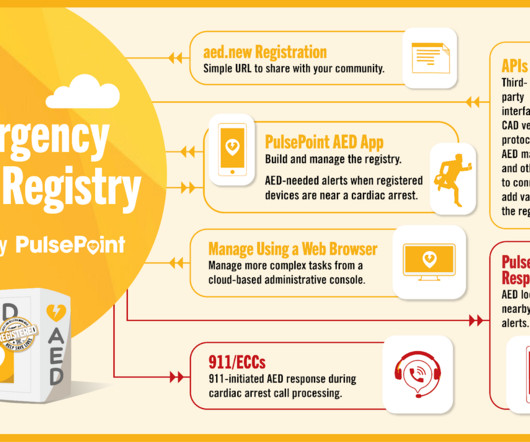
October is Sudden Cardiac Arrest Awareness month, so High Performance EMS and PulsePoint are encouraging everyone to locate and register Automated External Defibrillators (AEDs). By doing so you’re helping to build this network of life-saving devices. Every minute that a victim of Sudden Cardiac Arrest (SCA) goes without potential defibrillation, the chances of a responding EMS crew finding a shockable rhythm decrease between 7 and 10%.
Dispatching the right unit to an EMS call was much simpler when all resources had the same capabilities and a response time was the primary measure of success. It was a matter of determining which crew was available closest to the scene. Some computer-aided dispatch (CAD) software did better than others by considering the average travel time of an actual route instead of allowing nearness to be determined by a straight-line distance.
Sadly, this is not an adventure story of heroic first responder actions on the scene of an emergency incident but rather about how current EMS operations are failing us and their missions. Across the country, a quarter of positions in the dispatch center , the folks we rely on to keep resources coordinated, are going unfilled. Recent annual surveys also show that over 10% of EMS clinicians will leave the field entirely each year.
There is plenty of data in the world, the key to improving performance is to discover the right information and make an appropriate decision, based on facts, in time to change outcomes for the better. Computers are quite useful in aggregating and processing data to distill information in support of the decision-making process, but artificial intelligence and machine-learning has increased our expectations of cyber assistance.
The NHTSA Office of EMS released a significant document last year called the EMS Agenda 2050 that was carefully crafted to set a bold vision for the next 30 years of paramedicine by clearly differentiating the focus of care from its original definition in the 1996 EMS Agenda for the Future. Now, after just a few months of a COVID-19 pandemic, we have seen these modern precepts being challenged.
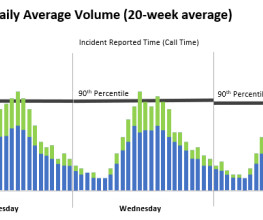
To know where our increasingly limited emergency resources will be needed next, we need to understand where future requests for service will originate. If we knew exactly where the next call would come from, we could proactively dispatch a resource there even before it is requested ( watch the movie “ Minority Report ” for an idea of how that might work. ) Unfortunately, the nature of emergency response is not nearly that easy, but that is not to say it is impossible to recognize use
I work regularly with agencies that are looking to improve aspects of their operations. Some casual readers may be surprised to know that the focus of those discussions is not always about cutting response times. While response is a simple and common measure, it clearly does not evaluate EMS well and certainly fails to encapsulate many of its complex needs and values.
I have often heard comparisons on the automation of System Status Management to the 2002 Spielberg movie starring Tom Cruise called “ Minority Report ” loosely based on the 1956 short story by Philip K. Dick. This science fiction action thriller is set in the year 2054 when police utilize a psychic technology to arrest and convict murderers before they commit their crime.
As we begin to wind down on the pandemic-level of constant 911 calls and the endless hours waiting on a room in the ED, we find ourselves in a time to reflect a little before our next call. Like so many services, we have a new influx of eager young professionals. Recently, a new student asked me, “ how do you guys keep doing this day after day ?” Not an unusual thing to ask lately, and my reply was this: “ determination and our perseverance to make sure our patient gets the definitive care and t
Elsewhere on social media this week I have seen a call to “protest EMS Week 2023” The logic suggests that the free meals and cheap trinkets are far less than the long-suffering and under-paid providers deserve. While I whole-heartedly agree, “we” have made EMS Week what it has become, not what it was intended. The EMS Week 2022 proclamation reads “I call upon public officials, doctors, nurses, paramedics, EMS providers, and all the people of the United States to obs
Dale Loberger FOR IMMEDIATE RELEASE: 9/13/22 BCS, Inc. (803) 641-0960 dloberger@bcs-gis.com BCS Releases MARVLIS Version 4.5 MARVLIS 4.5 Available Featuring Significant New Features and Updates Aiken, SC : BCS today announced the release of MARVLIS version 4.5. This major release provides new and updated features focused on our rapidly changing world.
I am pleased to announce the availability of my latest paperback book. As a consultant working with agencies across the nation that are representative of many distinct models of service, as well as being an EMS provider and a chief fire officer myself, I feel highly invested in the process to improve strategic dispatch and deployment decisions. It is my unique collective experience gained over more than 13 years of consultation and experimentation that is shared through these pages.
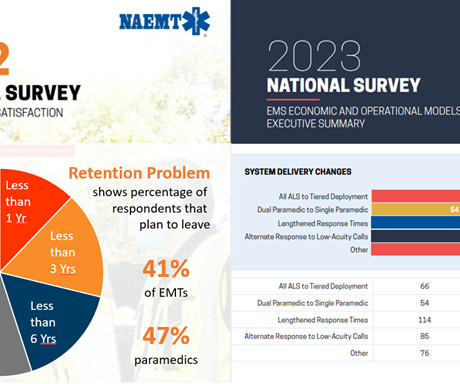
During the height of the COVID pandemic, shortages led to many operational challenges that required creative solutions. One of the more challenging issues that has become as endemic as the disease itself is the recruitment and retention of EMS professionals. This shortage has disproportionally impacted paramedics, as evidenced in the NAEMT survey results published in May of 2022.
Improvement of your deployment operations requires that you understand where your services will be needed and how to get the available units into the most suitable positions. Then, once you are prepared to respond, it is also critical that only the most appropriate assignments are made for each request to preserve your ability to respond to the next call as well.
Download the collaborative document created by several national professional organizations on “ Rethinking Emergency Medical Services.” There are several very quotable sections including, “The EMS staffing crisis highlights the need for reasonable, evidence-based and data driven system design and response changes to sustain these vital services while addressing the root causes of workforce shortages and economic challenges.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content