This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Kids get hurt. And they get sick. Its inevitable. Whether their fingers get caught accidentally in a car door or bedroom door slamming closed, or they trip and fall while running on their uncooperative little toddler legs , or catching all the germs as their immune systems slowly struggle to fight off every known virus to mankind. While most of the time, the injuries and illnesses are minor and self-resolving, every once in a while, there is major injury or illness, and significant bleeding is i
Kids have big heads relative to their bodies. Unfortunately with relatively big heads comes many traumatic injuries – think pediatric facial fractures , nasal fractures , tongue lacerations , ear lacerations , and dental injuries. The eye tends to unfortunately bear the brunt of some trauma , too. I’m looking at you hyphema and traumatic glaucoma !
As I have said before ( and I’m sure others of you have nodded along in agreement ), “ I hate rashes.” My disdain for rashes , however, only seems to ensure that every shift presents me with another opportunity to find clever and reassuring ways to say “ viral exanthem.” Clearly, not all rashes are related to viral infections (ex, DRESS , RMSF , HSP , Diaper Dermatitis ) and we have previously discussed an approach to pediatric rashes.
Diarrhea is one of the most common complaints in the pediatric emergency department, especially in the summer and early fall. Bloody diarrhea makes up approximately 15% of these enteritis presentations and though many causes are benign, some may be harboring something more insidious… Shiga Toxin-producing E.coli ( STEC ) and this may be associated with a terrible problem – Hemolytic Uremic Syndrome (HUS) !
We talk about a lot of common, not-to-miss diagnoses here at the Morsel Bakery, but we also talk about remaining vigilant for more subtle or uncommon diagnoses. We have spoken about causes to consider when working up a Fever of Unknown Origin including Myocarditis , Osteomyelitis , Acute Rheumatic Fever , and Lemierres syndrome. Today’s topic is a very uncommon diagnosis (estimated <5000 people in the U.S. with this disease, though likely under-diagnosed), but is worth talking about when c
Concussions are commonly encountered in the Emergency Department. We have previously discussed an approach to the question of when a patient “ can return to sport.” That recommendation has been revised ( calling for us to Rebake this Morsel ) and now also pays specific attention to the important aspect of scholastic activities. Let’s take a quick minute to digest a morsel on the current concussion in sport recommendations with respect to Return to Learn and Return to Sport : Re
Neonates presenting to the Emergency Department often cause a lot of uncertainty. Is this scalp swelling normal? Is this bloody stool concerning? Are this odd movements part of normal development? Is that umbilical area ok or concerning? Fortunately, we have addressed many neonatal issues in the PedEMMorsels. Obviously, one of the most concerning considerations in neonates is the potential for infection.
It’s never comfortable and is often very distressing to have skin problems and infections, such as intertrigo , folliculitis , panniculitis , omphalitis , or even preseptal or periorbital cellulitis. It’s even more distressing when the skin problem affects the penis. While summer is starting to wind down, and Summer Penile Syndrome is less likely to occur, we must still be vigilant for penile problems that can occur all year long.
We have discussed many causes of encephalitis and encephalopathy previously (ex, Eastern Equine Encephalitis , Posterior Reversible Encephalopathy , FIRES , Reye’s Syndrome ) and have highlighted the fact that they can be challenging to diagnose early. An irritated brain can lead to such a wide array of symptoms. It is even more challenging when the initial symptoms seem to align with what we perceive as psychiatric concerns.
Previously, we covered Post-Tonsillectomy Hemorrhage and how we hope that “all bleeding eventually stops: ideally, by means that we have imposed rather than by exhaustion of the patient’s RBC resources.” Since the original morsel ( way back in 2012 ), the literature has shown that there are a few extra ingredients that we can add to our morsel recipe when we care for children with post-tonsillectomy hemorrhage.
It seems like just yesterday ( or maybe ~ a month ago ) when we served up a tasty morsel on the PECARN decision rule for intra-abdominal traumatic injuries in children. Our friends at the PECARN injury group have remained busy this spring with generating more externally validated clinical decision rules. In addition to the recently published low risk intra-abdominal injury validation, we have another new tool to use this summer as school breaks, underdeveloped frontal lobes, and high speeds leav
The management of pediatric thermal burns always seems to be a hot topic , whether we are caring for a little future chef who splashed a scalding microwaved noodle cup on himself, or a toddling youngster who pulled a pot of boiling water on herself. Or maybe you have the adventurous adolescent who was a little too aggressive with the lighter fluid before igniting the campfire.
Ooooo the infamous chief complaint of “ weakness ” ……. We just love those don’t we? Although neurological complaints may not be a crowd’s favorite, it is one we must become comfortable with. Timely recognition and treatment can be life-improving and life-saving! So, with that goal in mind, let us digest another delicious morsel on weakness – Acute Transverse Myelitis in Children : Acute Transverse Myelitis in Children: Basics Rare, non-compressive, inflammatory condition of the spinal cord
Knowing how to manage a severe asthma exacerbation in the ER is a vital ingredient to being a successful ER doctor, but what about the more mild cases? The kids with a history of wheezing that are at the start of a viral URI but not yet in the midst of an exacerbation? What recommendations should we be giving these families? Lucky for us, in 2020 there were some updates made to the NIH Asthma Management Guidelines and we’re going to discuss which ones can help us in the Emergency Department!
Evaluation of unintentional injury and trauma is one of the hallmarks of the EM and PEM physician. One of the most difficult and most satisfying parts of pediatric emergency medicine is using one’s history, exam and clinical tools to make an informed decision and spare children from unnecessary pain , uncomfortable exams, painful procedures and medical imaging.
Children like to pretend to be grown-ups. Unfortunately, sometimes they develop grown-up problems ( Cholelithiasis , Kidney Stones , and Hypertension ). Additionally, often kids will complain of symptoms that warrant great concern in adults, but often engender apathy when considered in children. Chest Pain in Children is a great example of one of these complaints.
Trauma season is at hand and like all other pediatric emergency departments in the country, we find our ED breaking ( pun intended ) at the seams with orthopedic injuries. We see all different flavors of upper extremity injuries. Yes, we’re talking about your clavicular , proximal humeral, supracondylar, lateral condylar , scaphoid and metacarpal fractures.
Traveling Ticks are more than just ticking off a checklist before you get ready to travel! Climate change and changes in land usage have contributed to an expanded range of ticks (Beard 2016). There are species of ticks found on every continent and carrying a variety of vectors capable of infecting humans. Globally, ticks are the second most common vector to transmit illnesses after mosquitos (Parola 2018).
Often our job requires us to consider the presence of needles of significant illness in the haystack of nonspecific symptoms. With the help of our favorite geneticist , Dr. Liz Baker, we will dive into the haystack headfirst and find those needles. Hopefully, without getting poked. Let’s consider Inborn Errors of Metabolism Presenting in the ED : Inborn Errors of Metabolism: Basics Common Presentations, Uncommon Kiddos For the child with lethargy, vomiting, acidosis, hypoglycemia , organom
We encounter seizures commonly in the Emergency Department. While they can be dramatic and devastating, we have learned to become comfortable with the wide variety that may present in children. From the simple febrile seizure to the complex seizure, we know how to stabilize and how to evaluate. While fortunately most seizure activity is short lived, we also know that status epilepticus can be difficult to manage, and persistent seizures should make us consider specific etiologies (ex.
We have digested many Morsels regarding various pulmonary complaints. While some are very rare (ex, Pulmonary Embolism , Pulmonary Hypertensive Crisis , Negative Pressure Pulmonary Edema , CPAM ) others are commonly encountered (ex, Croup , Bronchiolitis , Sinusitis ). It is pneumonia , however, that often generates the most conversations. When should I consider a CXR ?
There have been many times I have encountered a triage note which states “ patient recently returned from … (insert awesome foreign country) … ” Not only does this leave me daydreaming about my future travel adventures, but has often caused me to take pause. Thoughts of what endemic illnesses could this child potentially have been exposed to in their travels?
If you have ever talked with a pediatric emergency medicine physician about some basic tenets of their practice, one of them will inevitably be, “ Never trust a neonate. ” The first few months of life outside the womb can elucidate a myriad of problems that were previously hidden during the prenatal state. We have previously touched on congenital issues like Congenital Adrenal Hyperplasia , Congenital Pulmonary Airway Malformation , Neonatal Leukemia , and of course there is always the Inconso
While doing literature review for my scholarly project it dawned on me that it might be time to dust off a classic morsel from the bottom of the cookie jar. On this 10 year anniversary, we chose to throw this one back in the oven to include some even more delicious data on cuffed endotracheal tube (ETT) use. No matter whether you have the wisdom of many years of practice ( old doc like Dr.
Imported Malaria , like all imported tropical illnesses, is a Tale of Two Cities. The infection was unknowingly obtained while enjoying a delightful holiday and then brought back in transit to a country where it is not endemic. In these non-endemic countries, we need to always be attentive to patient’s history of recent travel to correctly identify any concerns related to their recent travel.
Taking care of a critically ill child can be nerve-racking to say the least, and downright petrifying for those who don’t do it frequently, even if they are well-trained and brilliant clinicians. Dr. James Broselow, a family medicine-turned-emergency medicine physician from Hickory, North Carolina , recognized that his team spent a lot of time trying to calculate doses of medications rather than spending their mental energy on the actual medical decisions for the resuscitation.
Post-COVID everyone seems to be posting the perfect picture of their travels to the far reaches of the world. While this is an exciting change, it allows transmission of illness to countries where they are not endemic. Recently, a pediatric patient presented to the ED who just returned from abroad with a gastroenteritis presentation. In addition to my passion for PEM, I also share a passion for global health.
To celebrate the end of trauma season ( is it ever really over? ), we here at the Ped EM Morsels Bakery have cooked up a morsel to remind you that pediatric trauma can be even more difficult than you think. Never fear. As our fearless leader likes to say: “children are not aliens, but they are a special population with unique anatomy and physiology.” Children compensate for blood and volume loss very well… until they don’t.
Life is full of hazards! Chance encounters with life’s hazards seem to increase in the Summer time (ex, Trampolines , Snakes , Lawn Mowers , Water , and Heat ). It is good that continue to raise awareness of such hazards so we can prevent them ! Certainly, the care of pediatric patients is known for its “ Seasonality. ” Now that the long days of summer ( for us in the Northern Hemisphere ) might be behind us, some of those hazards may also be receding, but injuries and illnesse
While the “excitement” of the Emergency Department that is seen on TV may make people think that the only skills we need are those that help us manage Critical Illnesses or Traumatic Injuries , as we have digested in prior Morsels (ex, Developmental Milestones , Formula Primer , Vegan Diets ) all aspects of patient care are important for us to be adept at.
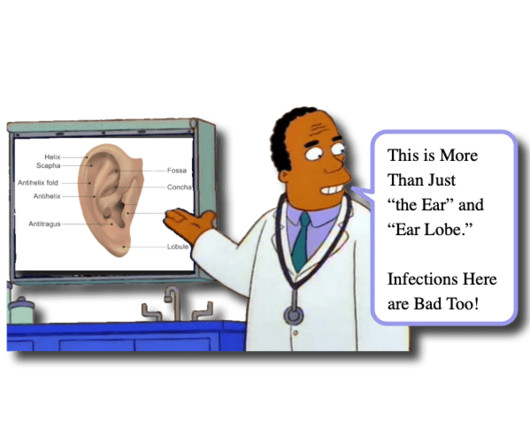
When you read the Morsel on Perichonditis of the ear last week ( or perhaps the Plantar Puncture Morsel from many many many weeks ago ) you may have objected because of the mention that, when indicated, fluroquinolones are safe in children. Some of you may have thought to yourself “first the AAP allows tetracycline ( Rocky Mountain Spotted Fever ) and now they allow fluoroquinolones use in children… what next?!
This is the 601st Ped EM Morsel ! Having authored 575 ( well, now 576 ) of them, I am often quite convinced that there are no new topics to discuss. Then July happens and we get 14 more amazing interns who help educate me and remind me that there is always more to learn. Recently, Dr. Teresa Crow encountered an important topic in children that deserves its own Morsel.
In the age of Ozempic, everyone seems to be losing weight! This seems to have had an overall positive benefit on the health of many. Losing weight is a good thing, until it is a bad thing! Too much of a good thing is a bad thing. Of course, there can be many complications of rapid weight loss including gallstones , malnutrition , and electrolyte imbalances.
Authors: Drs. Kendra Jackson and Rebecca Raffler While we’ve gotten to snack on a Morsel on this subject before , new guidelines and research surrounding DKA and cerebral edema have come to light since the first go ‘round! Thankfully, Dr. Fox wasn’t too “ salty” when we asked to rehydrate this topic. Rates of type 1 diabetes have increased since the COVID-19 pandemic.
In emergency medicine, we often use illness scripts and protocols to help drive our decision-making. I recall a shift I had with Dr. Fox while I was early in fellowship ( not so many years ago ). We had just received a young child from EMS who was post-ictal with decreased mentation. Dr. Fox asked me what I wanted to do next to care for the child, and as I calculated his GCS… 7 at the time… I felt somewhat obligated to say that I should intubate the child. “ Less than 8, intubate!
In the past, we have discussed several causes of Knee Pain in children. Some of those causes are benign (ex, Osgood Schlatter’s Disease ) while others are scary (ex, osteosarcoma ). Evaluating the limping child , though, requires us to ponder not only the common (ex, Toddler’s Fracture ), but also to be vigilant for the severe (ex, Septic Arthritis ).
I’m sure you can recall at least several parents who bring their children into the ED for concern of recurrent pneumonias. Often the parents focus on a possible underlying immunodeficiency. Fortunately, most commonly these pneumonias are due to viral infections, and we can often offer reassurances to the parent. The differential could also include aspiration , asthma , and bronchiectasis depending on the patient’s history.
The subcutaneous space is a vast region of potential space where things can collect. Sometimes this can be used to our advantage, like when we need to give subcutaneous fluids to a dehydrated patient without an IV, or when we need to give SQ medications for things like Sulfonylurea overdose , Hereditary Angioedema , or DVTs. Sometimes, however, these deeper layers of the subcutaneous space can collect dangerous infections , like Necrotizing Fasciitis.
When we think of severe hemorrhage in children, we typically think about trauma. Maybe injuries to the spleen or kidney come to mind. Perhaps thoughts of pelvic injuries or severe head injury dominate our considerations. Of course, we all have a healthy respect for post-tonsillectomy hemorrhage and we like to talk about Damage Control Resuscitation.
There are lots of animals that bite. Since we all inhabit the same beautiful world , and sometimes we humans overtake previous habitats of animals, we inevitably will cross paths with an animal that bites us. Usually, animals bite from fear or defense of their offspring ( ex, Brown Recluse ). Sometimes they bite because that’s how they feed (ie, mosquitoes Eastern Equine Encephalitis ).
Children love to trick us! Sometimes it is all in good fun and other times it is quite serious! They like to pretend to be well when they are truly sick ( remember to check that Cap Refill and to never trust a Neonate! ) and they often show us “odd” findings that are really normal (ex, Growth Plates, Primitive Reflexes ). They like to keep us on our toes so much, that even their cervical bones can deceive us.
There are many conditions that we would like to think belong only to the “ adult patient problem DDx; ” however, as we have discussed several times previously, pediatric patients can experience many “adult conditions” (see, Aortic Dissection , Kidney Stones , and Cholecystitis ). Those conditions usually have a substantial risk factor and one of the most risky of risk factors is Sickle Cell Disease !
Pediatric x-rays are challenging. Of course, we want children to grow, but those darn growth plates really make interpretation of their films difficult !! We have previously discussed how the surrounding ligaments and tendon are often stronger than the weakest part of the child’s bone necessitating our vigilance when addressing the pediatric extremity complaint (ex, Ankle Pain , Elbow Injury , Supracondylar Fractures ).
Our world has become inundated with the newest food and diet crazes. It seems like every social media persona provides “expert” opinions on the best way to nourish our bodies. Adults are one thing, but how does that translate to our growing, developing pediatric patients? Today we are focusing on vegan diets in children , and which nutritional deficiencies we need to remain vigilant to spot!
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content