This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
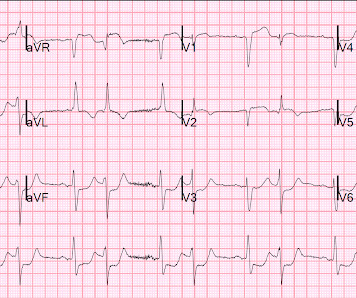
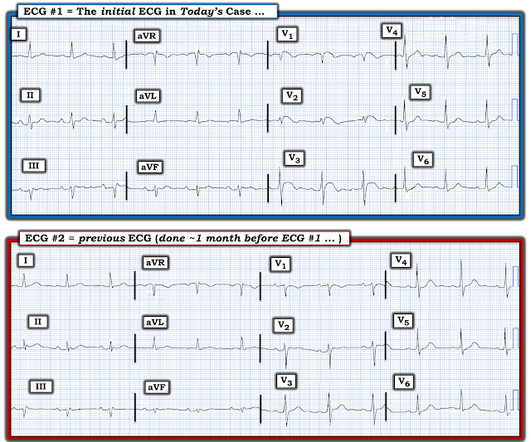
A middle-aged woman with known severe coronary disease had onset of substernal chest pain while at dialysis. A prehospital ECG was similar to the first ED ECG, which is shown below. Here is her initial ED 12-lead ECG: There is atrial fibrillation with a rate of approximately 114. Is this Acute Coronary Syndrome?
This is really good Prehospital, ED, and Cardiolog. Fever, tachycardia, hypotension, hypoxia and "SVT" A woman in her 40s with palpitations and chest pre. Flecainide toxicity 4/21/21 2597782 This case was flagged as a false positive cath lab. A man in his 60s with diaphoresis, vomiting, and i.
Acute coronary occlusion seen in paced *and* non-p. Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Danika Atrial fib RVR case in text message and inb. A 40-something male complains of worrisome chest p.
Ed Burns (from Life in the Fast Lane) sent me this. A 50-something with h/o coronary bypass has chest. See what happens when one fails to diagnose STEMI. Serial ECG recordings are essential: paramedic mak. Are These Wellens' Waves?? Repost this one great atrial tach case Early repol with increasing STE, formula values ve.
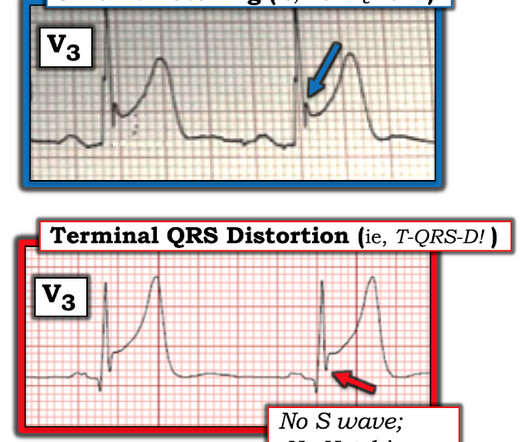
Emergency (ED placement) Transvenous Pacer appears. Back to basics: what is this rhythm? What are your. 30 yo woman with trapezius pain. HEART Pathway =. Good case for showing a flutter and LBBB, Good cas. What is this rhythm? Back to basics. Is there Terminal QRS Distortion? What is so unusual about this inferior OMI (which.
Intubated External pacing To cath lab Coronaries ok Pacemaker Posted by Steve Smith at 8:16 AM Email This BlogThis! Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them.
Dysnpea and Elevated troponin Takotsubo that looks like LVA Huge Precordial ST Elevation in an ED Patient Tachycardia, hyperthyroid, and ST elevation. Is this just right bundle branch block? Besides the Nonspecific T-wave Inversion in aVL, W.
Chest pain resolved, and a "Normal" ED ECG 2 cases of false pos STE aVL What will you do for this patient transferred to y. 30-something male with confusion, weakness, headac. A Patient with Respiratory Failure and a Computer. Cardiac arrest with STEMI pattern: no acute corona. How accurate are the Monitor leads for ST Elevation?
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
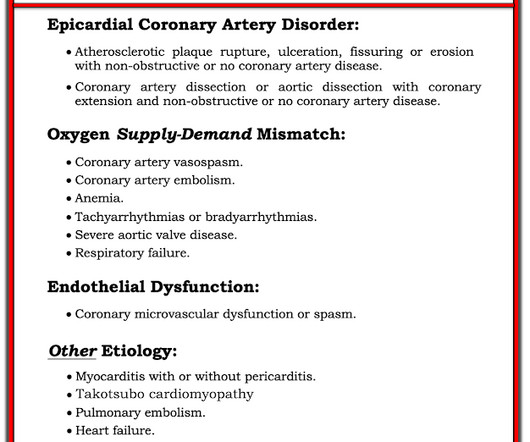
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
But the paramedic and the ED physician in this case did not subscribe to this idea. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. So this study is worthless and must be ignored.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Chou’s Electrocardiography in Clinical Practice, 6th ed. Goldberger’s Clinical Electrocardiography: A Simplified Approach, 9th ed. Attached is the first ECG.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. Asymmetric.
” – Musings of an American ED resident in July 2022 when US healthcare was affected simultaneously by supply chain issues from GE Healthcare (contrast media) and Abbott Laboratories (Similac baby formula). 3 A study of CT use trends in the ED has shown increasing use of CTs by almost 60% from 2005 to 2013.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? J Electrocardiol 2013;46:240-8 2.
She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Updates on the Electrocardiogram in Acute Coronary Syndromes. Current Emergency and Hospital Medicine Reports (2013) 1:4352. Electrocardiogram patterns in acute left main coronary artery occlusion. The patient was discharged neurologically intact.
et al, Emergency Medicine Clinical Essentials ed 2. Philadelphia: Elsevier, 2013 (Ch) 26: p. Eye Emergencies, in Tintinalli J et al (eds): Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, Seventh Edition New York City: McGraw-Hill 2016 (Ch) 241 Guluma K, Lee JE. 209-225 Walker R, Adhikari S.:
It is our job to identify this entity and ensure these patients receive the same care they would for a STEMI in any other coronary artery territory. Therein lies the limitation of electrocardiography in diagnosing acute coronary occlusion. Tips for recognizing Acute Posterior STEMI: 1. Neth Heart J. 2007; 15: 16-21. Wung SF, Drew BJ.
Resources REBEL EM: SVT with Aberrancy Versus VT Amal Mattu’s ECG Case of the Week: August 26th, 2013 ALiEM: Tricks of the Trade: Valsalva Maneuver By Using a 10cc Syringe Larry Mellick: Treating SVT with Adensoine ALiEM: Trick of the Trade: Combining Adenosine with the Flush References Brugada P et al. Am J Emerg Med 2011; 29(5): 545-8.
Int J Cardiol 2013 2. Identifying patients with low risk for acute coronary syndrome without troponin testing: validation of the HEAR score. High-sensitivity cardiac troponin I at presentation in patients with suspected acute coronary syndrome: a cohort study. Backus BE, Six AJ, Kelder JC, et al. Shin YS, Ahn S, Kim YJ.
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. In the cath lab, the patient’s blood pressure remained low.
Moreover, the research which appears to confirm this idea was indeed in relation to the circumflex, but they did not study Occlusion ; rather, they studied asymptomatic coronary disease. I showed conclusively that this is a common finding in normal ECGs, though it is more common in LAD Occlusion than in norml variant STE.
Along the way to acquiring more experience in recognizing the ECG findings of acute coronary occlusion — is incorporation of a number of KEY ECG Features into one's clinical acumen. Instead, the ST-T wave appearance may change in serial tracings recorded over the course of a single ED visit.
== MY Comment by K EN G RAUER, MD ( 8/22/2020 ): == The patient is a mid-50s man who presented to the ED for new-onset chest pain of ~1 hour duration. He was still having chest pain in the ED at the time ECG #1 was done ( Figure-1 ). The angiogram showed completely normal vessels ( No evidence of coronary disease! ).
Posterior STEMI" may not even technically exist according to the current (2013) ACC/AHA STEMI guidelines, as it is not described as a "STEMI equivalent" and the only relevant statement in the guidelines is: "In addition, ST depression in 2 precordial leads (V1-V4) may indicate transmural posterior injury." Comment from K. What is "STEMI"?
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. BP gradually rose. This ECG is diagnostic of diffuse subendocardial ischemia.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 He denied chest pain or shortness of breath. See below for PM Cardio digitized version of this.
Am J Cardiol 12(9):1379-1383; Nov 2013. Conclusion We might think about two reasons to be concerned with prolonged QT intervals in the ED. Still, absent data on how prevalent RR and QT pairs are in the ED, its hard to do better. Still, absent data on how prevalent RR and QT pairs are in the ED, its hard to do better.
Sex ed” sucks. A 2013 study found that half of young Australians are dissatisfied with school-based sex education. They believe that Sex Ed programs are irrelevant to real-life experience and contain inadequate discussion of important issues, including consent or positive sexual relationships. Why does it matter?
Some of the critical differentials include pulmonary embolism, acute decompensated heart failure, pneumonia, pneumothorax, and acute coronary syndrome. Anginal chest pain, chest heaviness, or evidence of fluid overload suggest acute coronary syndrome or acute decompensated heart failure. Signs and symptoms of systemic infection (e.g.,
The use of CTA (computed tomography angiography) in the emergency department (ED) has increased dramatically in the past 20 years. of all patients in the ED for over 800 different stated indications. 5, 6 Further, any use of imaging prolongs ED stays, which by extension increases ED wait times for other patients.
He arrived in the ED and had this ECG recorded: The first high sensitivity troponin I returned undetectable (3 ng/L). Myocardial Infarction with Non-Obstructive Coronary Arteries. Etiologies (list not comprehensive): Coronary Spasm. The cath lab was activated by the medics. So this is "MINOCA". Embolism with lysis.
The patient was accepted for emergent coronary angiography due to chest pain and ST-elevation. The coronary angiogram did not reveal any pathologic changes. Another ECG recorded after coronary angiography was unchanged from the initial tracing. High sensitivity troponin may increase slightly following coronary angiogram.
On arrival in the ED, a bedside ultrasound showed poor LV function (as predicted by the Queen of Hearts) with diffuse B-lines. Lidocaine had been used for the prevention of VF since the 1960s after coronary care units became a standard setting for the treatment of AMI. The paramedics diagnosis was "Possible Anterolateral STEMI."
Rates of occurrence of PIRP have decreased drastically in the era of percutaneous coronary intervention. Incidence and Prognosis of Pericarditis After ST-Elevation Myocardial Infarction (from the Acute Coronary Syndrome Israeli Survey 2000 to 2013 Registry Database). of patients developed PIRP [ 1 ]. Oliva et al. [ Hammill, S.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content