This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
2016; 83(1): 67-79. fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold Management of drug and alcohol withdrawal. N Engl JMed. 2003; 348:1786-1795. Cleve Clin J Med.
The characteristics that were significantly different between the LR and NS exposure groups race, organ dysfunction at presentation, ICU admission, hemoglobin SS genotype, discharge year, and hydroxyurea use were appropriately included as confounders in the TMLE analysis.
84 All patients with severe malaria need inpatient admission, ideally to the intensive care unit (ICU). International Monetary Fund; 2016. Centers for Disease Control and Prevention; 2016. Global, regional, and national burden of meningitis, 19902016: a systematic analysis for the Global Burden of Disease Study 2016.
A pilot randomized controlled study Journal of Critical Care Effect of Ketamine Analgosedation on Neurological Outcome in patients with Severe Traumatic Brain Injury: A Randomized Controlled Pilot Study Neurocritical Care Effects of a general practitioner-led brief narrative exposure intervention on symptoms of post-traumatic stress disorder after (..)
Lower intubation, need for BPAP and ICU admission in bolus group (Levy 2007). 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). versus 11.5%) and 12 hours (88.5%
Similar results were found for 219 paired samples from ICU patients with statistically significant but clinically meaningless differences for sodium and potassium ( Triplett 2016 ). for sodium ( Uysal 2016 ). Am J Emerg Med 2016; 34(3): 419-24. for potassium and 0.85 Acad Emerg Med 2011; 10: 1105-8.
Harder outside of an ICU setting) Therapeutic drainage of CSF? 2016 Jun;72 (6):768-769]. Hypertonic saline: Give a bolus 250 mL of 3%. Mannitol: Give 1.5 g/kg and then place a foley to track urine output and match the output with IV fluids. Not typically done in the ED. Recurrent LP or lumbar drain thats placed by neurosurgery.
6 Patients who receive deferoxamine, have significant metabolic abnormalities, or hypotension should be admitted to an intensive care unit (ICU). She was initiated on deferoxamine and admitted to the ICU. McGraw Hill; 2016. 1 Picture 1: Vin ros appearance of urine after treatment with deferoxamine. Hernandez SH, Nelson LS.
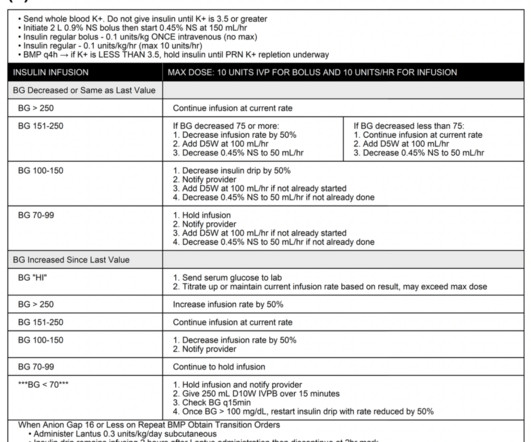
The patient states he has had multiple “diabetic emergencies” in the past and usually ends up in the intensive care unit (ICU) on a drip. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?” However, the ICU is full and the patient will likely be boarding in your ED for a bit before coming upstairs.
In our emergency department, the RTs do not spend a lot of time going around measuring cuff pressures and usually save that until the patient reaches the ICU. Published May 4, 2016. Hence, the RT’s are supposed to have them. Pearl 1: Check the units of pressure being used. Placement of a Blakemore Tube for Bleeding Varices.
NEJM Dec 2016 Guest Skeptic: Dr. Neal Little is an Emergency Physician who works at Chelsea Hospital in Chelsea, Michigan. NEJM Dec 2016 Guest Skeptic: Dr. Neal Little is an Emergency Physician who works at Chelsea Hospital in Chelsea, Michigan. [display_podcast] Date: November 27th, 2017 Reference: Legriel et al.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
Study Overview A recent research study titled “Sodium Bicarbonate Use During Pediatric Cardiopulmonary Resuscitation: A Secondary Analysis of the ICU-RESUScitation Project Trial” aimed to evaluate the associations between sodium bicarbonate use and outcomes during p-IHCA. 1.34; p = 0.621).
So with yet another confounding variable added (sicker patients at baseline in methylene blue group), the comparison of these two medications is yet again even more difficult There was no difference in ICU and hospital length of stays or hospital mortality between the two groups.
The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. 2016; PMID: 27720568 Guest Post By: Courney Knieriem, MD PGY-1, Emergency Medicine Resident RWJBH Community Medical Center, Toms River, NJ Courtneyknieriem.md@rutgers.edu J Med Toxicol. Epub 2019 Jul 3. Intensive Care Med.
The group that received phenobarbital had a higher maximum CIWA score than the group that received lorazepam, which could mean that phenobarbital was not as effective as lorazepam, although this is potentially confounded by patients who were transferred to the ICU were excluded from the study.
All patients who receive thrombolytics for ischemic stroke should be admitted to a neurosurgical, neurologic, or medical ICU for management and monitoring, as this is shown to decrease mortality and length of stay. doi: 10.1136/neurintsurg-2016-012515. Epub 2016 Jul 15. Neurocrit Care 24, 172–179 (2016).
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
ICU: 42.6% vs 0% ICU length-of-stay: 9 days vs 7 days In-Hospital Mortality: 28.2% ICU Mortality: 56.7% Conversely, it may be reasonable to withhold prophylactic platelets for patients in the ICU setting due to trends of lower bleeding risk noted as well as more intensive bleeding monitoring. Median hemoglobin: 8.2
Once upon time there was the AKIKI trial led by Gaudry and published in NEJM in 2016. Next enter the IDEAL-ICU trial by Barbar in 2018 which is yet another French multi centre RCT which randomised septic shock patients to CRRT or not at 12 hrs after meeting the F on the RIFLE criteria.
Enrolled 800 fairly typical ICU patients, and found a 35% vs 39% mortality benefit favouring the vaso but of course this was below the somewhat arbitrary statistical significance. A somewhat underwhelming start Second is the VANISH trial by Gordon et al, JAMA 2016. This was closer to home in the UK, with 18 ICUs. Gordon, A.
2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). Based on 2019 American Heart Association (AHA) guidelines, amiodarone and digoxin have been suggested as alternative options in controlling ventricular rate refractory to first-line BBs and non-DHP CCBs.
Lancet August 2016. Lancet August 2016. Lancet August 2016. Outcome: * Primary: In-hospital mortality at initial hospital or secondary hospital if transfer occurred * Secondary: 24 hour and 30 day mortality, imaging time, time to diagnosis, length of stay (LOS) in the trauma room or ICU, number of days of mechanical ventilation.
Studies without IRB approval Studies older than 2016 Intervention: Administration of <30 mL/kg IV crystalloid fluids within three hours of sepsis identification. Secondary Outcomes: Delayed hypotension, increased ICU stay, and other relevant outcomes. Outcomes: Primary Outcome: In-hospital mortality.
They consecutively enrolled 1,817 ICU patients from 45 sites across China. Population: Inclusion Criteria: Age 18-75 years old SOFA score 2-13 Admitted to the ICU with a diagnosis of sepsis 3.0, “ Life-threatening organ dysfunction caused by a dysregulated host response to infection.” 002) ICU-free days: Placebo 12.4%
Removed from cooling at 102 and admitted to ICU. 2016 study published in American Journal of Emergency Medicine , “ Urinary obstruction is an important complicating factor in patients with septic shock due to urinary infection ” by Reyner et al. 2016 Apr;34(4):694-6. Cooling blanket placed, but temperature increases to 107F.
This has relevance to the ICU population in 2 major ares * Sepsis. * EF does not correlate with particularly well with mortality in sepsis though diastolic dysfunction does * It may be due to under filling and the reduced diastolic filling due to the ubiquitous tachycardia in sepsis.
2016) “Implementation of a Post-Code Pause: Extending Post-Event Debriefing to Include Silence”. 2018) “Sacred Pause Imitative in the ICU: A survey of ICU physicians and nurses”. Be kind and care for yourself and those around you. Please watch this video for a beautiful explanation from Jonathan Bartels of this initiative.
What They Did Single-center randomized controlled study design performed by the Department of Hepatology & Liver transplantation in New Delhi Study participants, investigator clinicians, data collectors, and data analysts were blinded Investigators recruited participants from February 27, 2016 – March 3, 2018.
An example using a real case I had while on call in the ICU: A 61-year-old female had a post-induction arrest on the wards/hospital telemetry floor after being intubated for airway protection. Epub 2016 Jun 28. In a PCAC 1 or 2, we may prioritize a cath and tolerate a couple hours without ICU Neuroresuscitation. Resuscitation.
1 This is a change from the 2016 SSC guidelines which suggested against corticosteroids. Disposition The SSC guidelines suggest that patients with septic shock or critical illness be moved to the intensive care unit (ICU) within six hours of presentation to the ED. Restriction of Intravenous Fluid in ICU Patients with Septic Shock.
The incidence of dynamic LVOTO in those with septic shock is remarkably high and is reported to be 20% in one study from ICU echo guru Michel Slama. Left ventricular outflow tract obstruction in ICU patients. Current Opinion in Critical Care 22 , 260–266 (2016). Critical Care 19 , 1–8 (2015). Tribouilloy, C. & Pollick, C.,
They found NO difference in drain failure rates ( 11% pigtail vs 13% chest tube P=0.74), total daily volume drained or length of ICU stay between groups. A recent review was conducted on Trauma Quality Improvement Program data between 2014 and 2016. Injury 2016; 47: 797– 804. Laan DV, Vu TD, Thiels CA et al.
Despite the risk of hypotension and bradycardia, propofol has been shown in the ICU setting to be a safe and effective monotherapy intubation agent for hemodynamically unstable patients (19). 2016 Sep;117 Suppl 1:i9-i13. Etomidate is likely an agent of last resort for monotherapy due to the short duration of action (12). 2021): e12373.
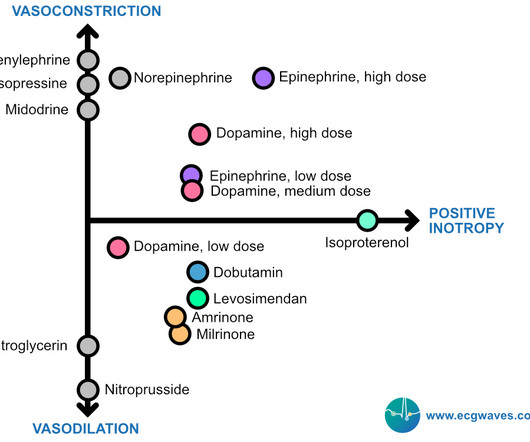
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). JAMA 2016; 316:509. Several endogenous and synthetic agents exist and are frequently combined to achieve the desired hemodynamic outcome. Most agents exhibit both vasopressor and inotropic effects (Figure 1).
Duration of mechanical ventilation, ICU, and percentage of vasopressor use were not significantly different. What They Did Prospective, randomized 1:1, parallel-assignment, open-label, single-center trial Randomization process: Sequentially numbered opaque, sealed envelope in blocks of 8 that directed the team to use either etomidate (0.2
There was no difference in the secondary outcomes of time to hemostasis, ventilator-free days, ICU-free days, disposition at 30 days, incidence of primary surgical procedures, and functional status at hospital discharge (measured as Glasgow Outcome Scale-Extended Score). 2016 May 1;202(1):182-7. vs. 78.1%, p=0.006). Ann Emerg Med.
In this situation, an ABG should be obtained periodically for correlation, though this is more relevant for the intensive care unit (ICU) setting than in routine ED care (5, 9). Epub 2016 Jun 9. 2016 Feb;33(2):152-4. Are there circumstances where ABGs are necessary, and why may consultants specifically request them? Emerg Med J.
Answer : Cardiac Transplant Complications Epidemiology: There were over 3,000 heart transplants in North America in 2016. Cardiogenic shock in the setting of acute rejection would warrant inotropic agents and ICU admission (C) , but these would not be indicated in cases of mild rejection, such as in this patient.
All treatments were given for the assigned time frame or until ICU discharge, whichever came first. In the control group, patients treated for severe sepsis or septic shock in the year prior to the initiation of triple therapy, hydrocortisone was used at the discretion of the intensive care unit (ICU) attending. 2016:316(17);1775-85.
2016 Dec;91(12):1185-1190. Epub 2016 Oct 3. May substitute levofloxacin if allergic to cephalosporin Anti-viral medications if indicated Oseltamivir for influenza Patients >14 days old Remdesivir for COVID Patients >28 days old and at least 7lbs (3.2 Am J Hematol. PMID: 27543812.
." When a critical care team transports a patient from an outlying ER to your ICU, do you automatically set your own ventilator settings, or do you ever use the vent settings the critical care transport team had dialed in for transport? "That’s We don’t seem to see Ketamine infusions in the ICU often. Why is that? "Ketamine
Let’s take a trip way back to 2016. LVEDP (measured in the ICU using a Swan-Ganz or pulmonary artery catheter) is the pressure inside the left ventricle at the end of diastole, when the LV is at its fullest. You’re me, and you’re in paramedic school, in the thick of the cardiology section. LVEDP is a little more complex.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content