This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
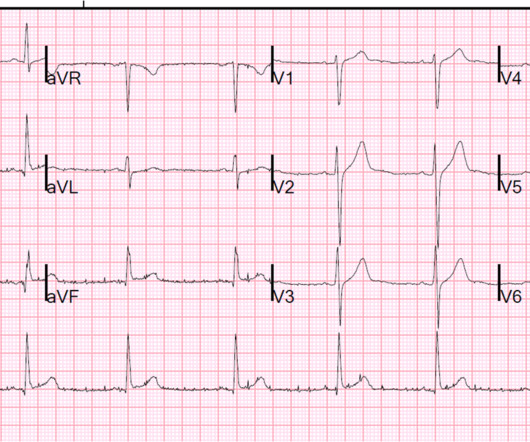
This dynamic change is diagnostic of ACS. Cardiology was consulted and agreed that his history was high risk for ACS and a next-day angiogram was merited. This was also non-diagnostic for OMI, although the dynamic changes are diagnostic of ACS. ECG at time 82 minutes: What do you think?
DOI: Papudesi BN, Malayala SV, Regina AC. This month in JAAD Case Reports: August 2023: Xylazine and skin necrosis. Journal of the American Academy of Dermatology. 2023 Aug 1;89(2):231. Xylazine toxicity. 2023 [book]. PMID 37603662 Rose L, Kirven R, Tyler K, Chung C, Korman AM. JAAD Case Reports. 2023 Jun 1;36:113-5.
Pain episodes, or vaso-occlusive crises (VOC), are a hallmark of sickle cell disease, often leading to prolonged hospital stays and serious complications like acute chest syndrome (ACS). While small studies suggest that early pain relief can shorten hospitalisation, the evidence remains limited.
3) ACS with possible additional ischemia from atrial fib with RVR 4) Hemorrhage/dehydration/sepsis/etc., I was fairly certain that this was a type II (demand ischemia) MI and that this patient was not having ACS. He did not have ACS. Not all myocardial infarction is due to ACS 2. He was treated for urosepsis and did well.
CT) Steroids and antibiotics for grade 2 or higher Dermatologic: 40-50%; local vs. severe (SJS/TEN/DRESS) Topical vs. systemic steroids Endocrine: 17%; hypophysitis (pituitary gland inflammation), hypo- or hyperthyroidism, diabetes, adrenal insufficiency Renal: 30%; AKI, glomerulonephritis, IgA nephritis, interstitial nephritis Pyuria, hematuria, hypertension, (..)
Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. PMID: 28106307 Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. To assess the clinical impact and relevance of these concerns, Alwang et al. performed the retrospective cohort study below ( Alwang 2024 ). JAMA Intern Med. 2024;184(11):1365-1372. Microcirculation.
ACS is dynamic. interesting spontaneous reperfusion case 1413140 prehospital STEMI first ED ECG is here, with 3/10 pain: But this is the same patient just 10 minutes before, with 7/10 pain Isn't it ridiculous to say that the patient has both a STEMI and an NSTEMI? It can't be given one static name. Now the patient has one disease: OMI.
link] Hummell AC, Cummings M. Accessed October 5, 2024. link] Centers for Disease Control and Prevention (U.S.). History and Physical: Refugee Health Domestic Guidance.; Accessed October 5, 2024. Role of the nutrition-focused physical examination in identifying malnutrition and its effectiveness. 2022;37(1):41-49. doi:10.1002/ncp.10797
.” Leveraging the ESO Patient Registry During an American College of Surg eons S ite Survey, presented by Matthew Derkrikorian, Trauma Program Manager at Rady Children’s Hospital, offered a look at how Rady Childrens Hospital prepared for and completed the first ACS Site Survey using ESOs updated registry. shared key takeaways.
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
It is important to note that these findings, if due to atherothrombotic acute coronary syndrome (ACS), are NOT due to occlusion of the left main, as is frequently stated in online postings and in literature. It is most commonly due to demand ischemia, not due to ACS! If it were ACS, what reperfusion options were available?
One must remember that acute pulmonary edema is frequently triggered by ACS. In this case, it is reasonable to assume that there is no ACS. Here is the troponin profile: Troponins this high are almost always due to type 1 MI (ACS, plaque rupture) This was a surprise. Severe, life threatening ACS may have no ST Segment shifts.
May mimic ACS Lesson : 1. And such absence may or may not lead one to pursue other diagnoses. Remember that Pulmonary Embolus: 1. Causes anterior T-wave inversion plus T-wave inversion in III 2. Often has elevated troponin 3. Often has elevated BNP 4. What appears to be pulmonary edema on chest X-ray may, in fact, be infarct or infiltrate.
ACS Chemical Neuroscience, 15(21), 3874–3883. References 1. de Andrade Horn, P., Berida, T. Bouchard, J. Jayakodiarachchi, N., Schultz, D. Lindsley, C. & Crowley, M. Classics in Chemical Neuroscience: Medetomidine. doi.org/10.1021/acschemneuro.4c00583 Centers for Disease Control and Prevention.
Causes: ACS, arrhythmia, valvular dysfunction, infection, nonadherence to meds, myocarditis, volume overload. In SCAPE, uncontrolled sympathetic function and increased afterload leads to HTN and fluid redistribution from the periphery into the pulmonary system. What are the key tests? Tests: ECG , labs, chest imaging.
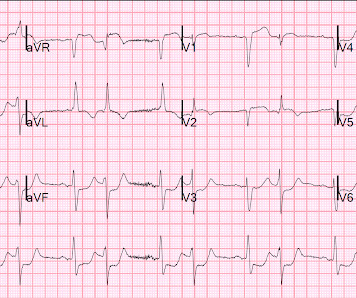
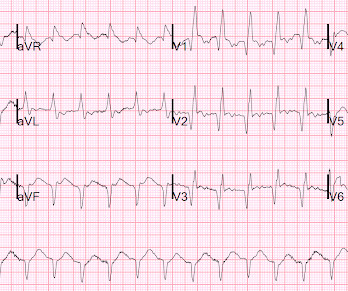
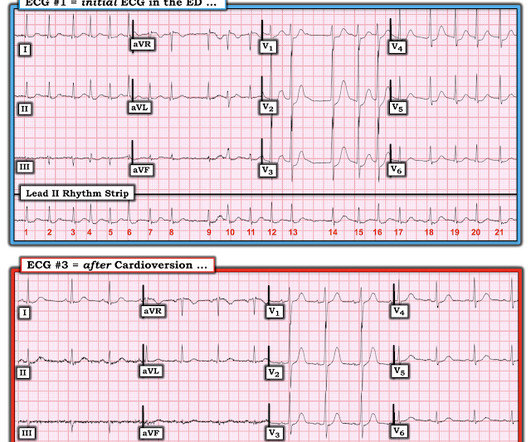
The history is highly suggestive of ACS. The patient was given a diltiazem bolus and drip, her pulse slowed, and her chest pain completely resolved. Another ECG was recorded: Atrial Fib with a controlled rate The ST Depression is mostly resolved with this slower rate The first troponin was, not surprisingly, elevated at 1.07
25 AC = Anterior chamber, ELISA = enzyme-linked immunosorbent assay, NS = normal saline, PCR = polymerase chain reaction Management Oral Ivermectin 26 150 mcg/kg given once or twice yearly for 10 to 15 years to match the lifespan of the adult worm is the standard treatment.
Blood sampled from existing peripheral IV cannulae yields results equivalent to venepuncture: a systematic review [ 10.1177/2054270419894817 ] Second Line 18 G Should we be placing in the AC? Future Show: Upping your IV Game Fluids Get dinged for 4, rectal temps on elderly, etc.
Govindraj R, Binda DD, Harris AC et al. Experiences of Racial Microaggression Among Migrant Nurses in the United Kingdom. Glob Qual Nurs Res. 2014 Jun 3;1:2333393614532618. doi: 10.1177/2333393614532618. PMID: 28462288; PMCID: PMC5342848. MedEdPORTAL. 2024 Sep 17;20:11435. doi: 10.15766/mep_2374-8265.11435.
. * Basic filters on the EEG include the high and low pass filters (should be LFF of 1 hz, HFF ~78 hz), and potentially a notch filter for 60 hz (in the US) or 50 hz (in Europe) to filter out AC electrical noise. Dark vertical lines on the strip occur every 1 second. Odd numbered leads are on the left side of the head.
One study found that the best discrimination of stress cardiomyopathy from ACS was possible with the ratio of NT-proBNP/cTnT on the 2nd day. and an accuracy of ∼96% in detecting stress cardiomyopathy as opposed to ACS. NT-proBNP and CTnT in ACS and Takotsubo) Smith : However, this is not of any help with the acute diagnosis!
Crowe L, Young J, Smith AC, et al. Parents’ prioritised outcomes for trials investigating treatments for paediatric severe infection: a qualitative synthesis. Archives of Disease in Childhood 2019;104(11):1077. doi: 10.1136/archdischild-2019-316807 20. Intensive and Critical Care Nursing 2023;78:103476. doi: [link] 21.
Learning Point: When there is ST depression and atrial fibrillation with RVR, it is very useful to cardiovert if possible, or slow AV conduction, before assuming that the ST depression is a result of ACS. == MY Comment by K EN G RAUER, MD ( 6/16/2020 ): == Interesting case presented by Dr. Smith — regarding this 60-something year old man who presented (..)
When seeing a South Asian patient with chest pain, concern for ACS must be heightened, given their disproportionately higher risk of CAD, despite often lacking traditional risk factors.) Patient initially presented at 9 PM to a referring facility with hsTnI 13 (ref: < 34 ng/L) then 30, then 60.
Katheria AC, et al. Misaligned Attitudes and Perceptions Among Adolescents Living With Obesity, Caregivers and Healthcare Professionals: ACTION Teens Australia Survey Study. Kwok C, et al. J Paediatr Child Health. 2025 Jul 14. Deferred Cord Clamping With High Oxygen in Extremely Preterm Infants: A Randomized Clinical Trial. JAMA Pediatr.
0318502 Lorenzi-Filho G, Genta PR, Figueiredo AC, Inoue D. Respiratory rate and its associations with disease and lifestyle factors in the general population – results from the KORA-FF4 study. 2025;20(3):e0318502. doi:10.1371/journal.pone.0318502 CHEYNE-STOKES RESPIRATION IN PATIENTS WITH CONGESTIVE HEART FAILURE: CAUSES AND CONSEQUENCES.
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
10 g/dL in patients with acute coronary syndrome (ACS). A restrictive strategy is one in which transfusion of packed red blood cells (pRBC) is administered at a threshold of 7-8 g/dL or 8.5-10 16 Provide adequate volume resuscitation as described above to correct the underlying cause of lactic acidosis.
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
They show that if there is not >/= 1 mm STE in aVR, then ACS is highly unlikely to be due to severe 3-Vessel disease or Left Main. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol;107(4):495-500. why is this important?
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
The ED physicians were of course worried about ACS, and they obtained these POCUS echos: Apical 4 chamber Overall LV function is moderately decreased Parasternal short axis: Is there an anterior wall motion abnormality? Parasternal long axis: Again, decreased LV function 101.8 WBC 27,000 0.299 trop UA with infection lactate 3.4
Big changes are on the horizon for trauma centers participating in the American College of Surgeons (ACS) Trauma Quality Programs (TQP). We’ve been working closely with the ACS to prepare for this transition. The ACS is aware that we are not updating the legacy registry products. What’s changing?
Credits & Suggested Citation Episode written by Avi Cooper Show notes written by Avi Cooper and Giancarlo Buonomo Audio edited by Clair Morgan of nodderly.com Cooper AZ, Abrams HR, Breu AC, Buonomo G, Manna, M. Wherefore Iodine? The Curious Clinicians Podcast. July 23rd, 2025. Image Credit: Wikimedia Commons
(4) Myocardial Injury - Chronic (1) Myocarditis (19) NOT-pseudonormalization (3) NSTEMI (6) NSTEMI is worthless term (1) Negative U-wave (1) New LBBB (12) New sign of LAD occlusion (1) No Reflow (10) Non-Occlusion MI (NOMI) (1) NonSTEMI (8) Noncompaction cardiomyopathy (1) Norepinephrine (1) Normal ECG by computer algorithm (54) Normal ECG in OMI (3) (..)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content