This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
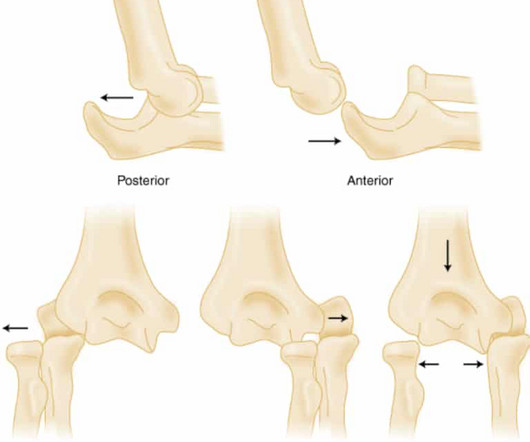
PMID: 32644703 Robinson PM, Griffiths E, Watts AC. PMID: 27227986 Glover NM, Black AC, Murphy PB. Commentary on an article by Marc Schnetzke, MD, et al.: “Determination of Elbow Laxity in a Sequential Soft-Tissue Injury Model. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. Simple elbow dislocation. 2023 Nov 5.
To assess the clinical impact and relevance of these concerns, Alwang et al. Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. PMID: 28423290 Kidwell K, Albo C, Pope M, et al. PMID: 24066745 Self WH, Semler MW, Wanderer JP, et al. PMID: 29485926 Semler MW, Self WH, Wanderer JP, et al. JAMA Intern Med.
57 Adapted from: Long B, MacDonald A, Liang SY, et al. link] Rother B, Pierre G, Lombardo D, et al. link] Hummell AC, Cummings M. link] Franco JR, Cecchi G, Priotto G, et al. Biggs H, Behravesh CB, Bradley KK et al. doi:10.1136/bmjgh-2018-001114 Okesanya OJ, Olatunji GD, Kokori E, et al. 57 Table 2.
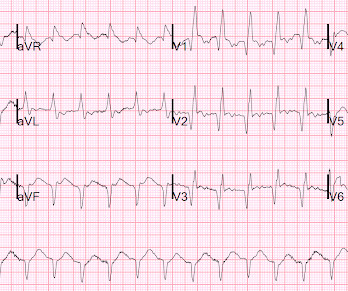
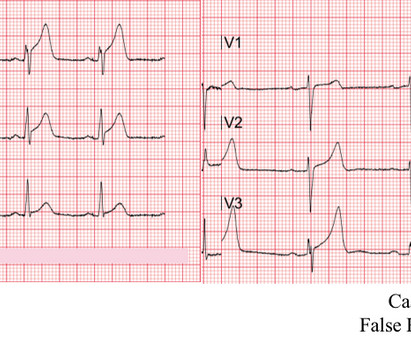
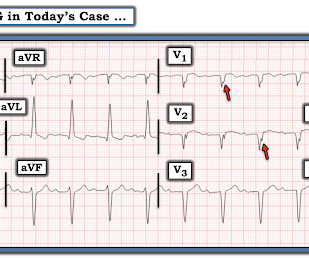
See this photo of Figure 1 in Wellens' first paper (de Zwann C et al. May mimic ACS Lesson : 1. This is spite of the fact that the T-wave inversions are atypical for Wellens' waves: pattern A has slight ST elevation with upward sloping ST segment, then sudden downward drop; pattern B has deep symmetric T-waves.
100% seems too good to be true Morello et al., Clin Exp Allergy. 2024 Oct 9. doi: 10.1111/cea.14565. Epub ahead of print. PMID: 39383344 Profundus Trial – Can we actually exclude acute aortic syndromes with this protocol? Diagnosis of acute aortic syndromes with ultrasound and D-dimer: the PROFUNDUS study. Emerg Med J. Epub 2018 Oct 25.
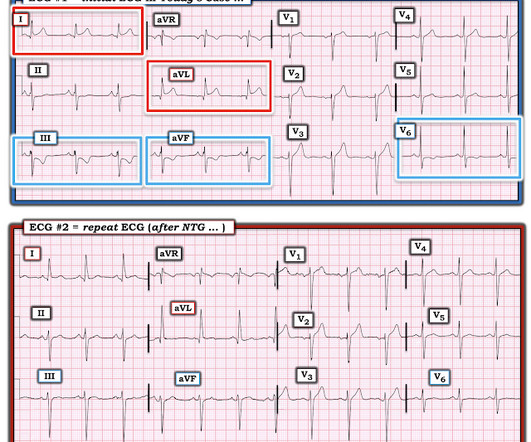
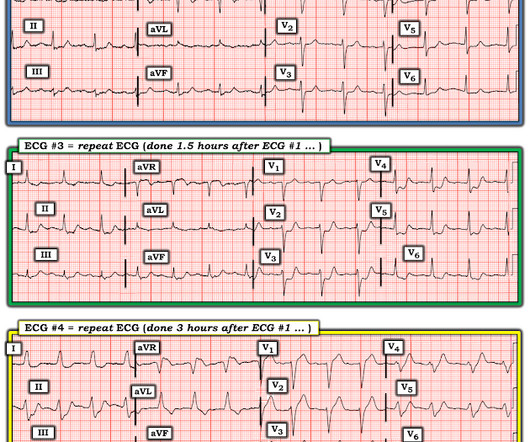
One must remember that acute pulmonary edema is frequently triggered by ACS. In this case, it is reasonable to assume that there is no ACS. Here is the troponin profile: Troponins this high are almost always due to type 1 MI (ACS, plaque rupture) This was a surprise. Severe, life threatening ACS may have no ST Segment shifts.
ACS Chemical Neuroscience, 15(21), 3874–3883. References 1. de Andrade Horn, P., Berida, T. Bouchard, J. Jayakodiarachchi, N., Schultz, D. Lindsley, C. & Crowley, M. Classics in Chemical Neuroscience: Medetomidine. doi.org/10.1021/acschemneuro.4c00583 Centers for Disease Control and Prevention. Thomas, S.
Open-access image reference: By Giovanni Maki, derived from a CDC image at [link] – Basáñez M-G, Pion SDS, Churcher TS, Breitling LP, Little MP, et al. Ehrlich JR, Ramke J, Macleod D, et al. link] Vinkeles Melchers NVS, Stolk WA, Van Loon W, et al. 0009604 Taylor MJ, Awadzi K, Basáñez MG, et al. volvulus life cycle.
Available from: [link] Desai V, Hernandez Conte A, Nguyen VT et al. Govindraj R, Binda DD, Harris AC et al. Workforce Race Equality Standard: 2020 Data Analysis Report for NHS Trusts and Clinical Commissioning Groups. February 2021. Veiled harm: Impacts of Microaggressions on Psychological Safety and Physician Burnout.
One study found that the best discrimination of stress cardiomyopathy from ACS was possible with the ratio of NT-proBNP/cTnT on the 2nd day. and an accuracy of ∼96% in detecting stress cardiomyopathy as opposed to ACS. Rallidis Et al. This patient never had ACS. A cut-off value of NT-proBNP/cTnT ratio >7.5
van Hasselt TJ, Gale C, Battersby C, et al. van Hasselt TJ, Kanthimathinathan HK, Kothari T, et al. Wilkinson K, Freeth H, Mahoney N, et al. Weiss SL, Peters MJ, Alhazzani W, et al. Darnell R, Brown A, Laing E, et al. Peters MJ, Ramnarayan P, Scholefield BR, et al. Peters MJ, Gould DW, Ray S, et al.
When seeing a South Asian patient with chest pain, concern for ACS must be heightened, given their disproportionately higher risk of CAD, despite often lacking traditional risk factors.) Transient STEMI was studied by Lemkes et al. Lemkes JS, Janssens GN, van der Hoeven NW, et al. Available from: [link] Lemkes et al.
Efrem E, et al. Maria Giovanna P, et al. Cristofori F, et al. Derbie AY, et al. Beard LA, et al. Piske M, et al. Pratt MTG, et al. Drummond H, et al. Assaad MA, et al. Dokousli V, et al. Daves G, et al. Heldbjerg AR, et al. Sanchez LM, et al. Pediatrics.
doi:10.1056/NEJMra1802529 Berry RB, Budhiraja R, Gottlieb DJ, et al. 2172 Fleming S, Thompson M, Stevens R, et al. doi:10.1016/S0140-6736(10)62226-X Rückert-Eheberg IM, Steger A, Müller A, et al. 0318502 Lorenzi-Filho G, Genta PR, Figueiredo AC, Inoue D. 160357 Lavonas EJ, Akpunonu PD, Arens AM, et al. The Lancet.
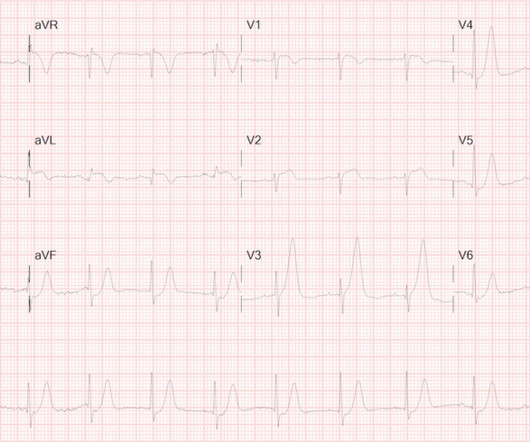
65 y old male, hypt, IHD, smoker, central chest pain, was in pulm oedema Killip III Great recent article relevant to this: Kosuge M, Ebina T, Hibi K, et al. They show that if there is not >/= 1 mm STE in aVR, then ACS is highly unlikely to be due to severe 3-Vessel disease or Left Main. Am J Cardiol;107(4):495-500.
Scientific Opinion on the re‐evaluation of Allura Red AC (E 129) as a food additive. Refined exposure assessment for Allura Red AC (E 129). .” Heliyon (2024). From FDA News release “HHS, FDA to phase out petroleum-based synthetic dyes in nation’s food supply” released April 22,2025 [link]. Ardila-Leal, Leidy D.,
Merz LE, Osei MA, Story CM, et al. Credits & Suggested Citation Episode written by Tony Breu Show notes written by Millennium Manna and Tony Breu Audio edited by Clair Morgan of nodderly.com Breu AC, Abrams HR, Buonomo G, Cooper AZ, Manna M. Development of Duffy Null–Specific Absolute Neutrophil Count Reference Ranges.
Davidson JS, Brown DJ, Barnes SN, et al. West S, Andrews J, Bebbington A, et al. Symons S, Rowsell M, Bhowal B, et al. J Pediatr Orthop. 2018;Volume 00(00):DOI:10.1097/BPO.0000000000001169. 0000000000001169. Simple treatment for torus fractures of the distal radius. J Bone Joint Surg Br. 2001;83:1173-5. Pediatr Emerg Care.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. years, with the interval as long as 12 or 18 years in some studies. Nor was there a challenge to look for coronary spasm.
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” ACS is usually amongst this differential, as cardiovascular disease is a leading cause of morbidity and mortality in this population. Reference: Wang et al. The utility of troponin testing to diagnose or exclude ACS. *
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
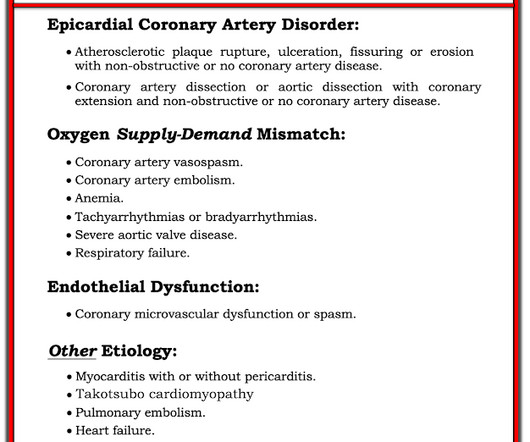
As per my review of this subject ( Check out My Comment at the bottom of the page in the November 16, 2023 post in Dr. Smith's ECG Blog ) — the 3 most common Causes of ACS ( A cute C oronary S yndrome ) with a "negative" cath are: i ) Myocarditis; ii ) Takotsubo cardiomyopathy; and , iii ) MINOCA.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. link] [1] Zachary et al. 2] Costanzo, L.
Date: June 30th, 2022 Reference: McGinnis et al. Date: June 30th, 2022 Reference: McGinnis et al. If we thought about ACS, we brought them in. Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. AEM June 2022. AEM June 2022.
Reference: Brichko et al. Reference: Brichko et al. Reference: Brichko et al. Chris Bond is an emergency medicine physician and assistant Professor at the University of Calgary. He is also an avid FOAM supporter/producer through various online outlets including TheSGEM. AEM Feb 2021. AEM Feb 2021.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Lindahl et al. From Gue at al. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data.
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. Reference: Broder et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the Emergency Department.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Heitner et al. For this test it is VERY low (very good) at 4% at the 99th percentile -- 26 ng/L, but it will not be so good at a level of 9 ng/L. The troponin is trapped in the myocardium that is not being perfused.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. EMRAP HD: Epistaxis Posterior Pack References Cassisi NJ et al. PMID: 5569677 Zeyyan E et al. PMID: 20938948 Loftus BC et al.
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. Am J Emerg Med.
doi:10.1093/tropej/fmz071 Expert Panel on Pediatric Imaging, Trofimova A, Milla SS, et al. 2019-0134 Hirtz D, Ashwal S, Berg A, et al. Riviello JJ Jr, Ashwal S, Hirtz D, et al; American Academy of Neurology Subcommittee; Practice Committee of the Child Neurology Society. J Trop Pediatr. 2020;66(3):299-314. J Am Coll Radiol.
Antonaci L, et al. Tritos NA, et al. Levi M, et al. Fishbein MH, et al. Cetinkaya PG, et al. Niu T, et al. Verkuijl SJ, et al. Varni JW, et al. Dias FC, et al. Peter C, et al. Ahlberg R, et al. Shir A, et al. Kuypers KLAM, et al. Hegeman EM, et al.
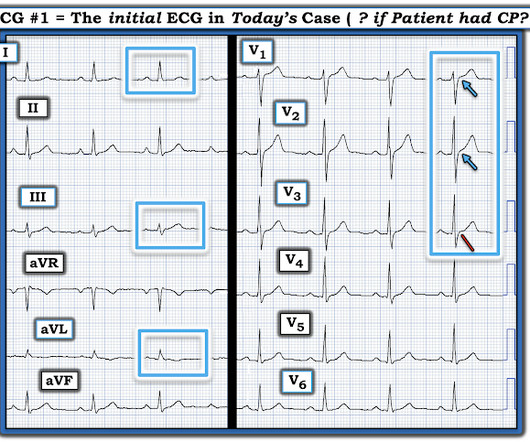
The original term " benign early repolarization" has fallen out of favor since the seminal paper by Haïssaguerre et al. As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). per 100,000 to 11 per 100,000 [Rosso].
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. But only 6.4% link] References 1.
Growdon ME, Jing B, Morris EJ, Deardorff WJ, Boscardin WJ, Byers AL, Boockvar KS, Steinman MA. Credits & Suggested Citation Episode written by Tony Breu Show notes written by Giancarlo Buonomo and Tony Breu Audio edited by Clair Morgan of nodderly.com Breu AC, Abrams HR, Cooper AZ, Buonomo G. J Am Geriatr Soc. October 2nd, 2024.
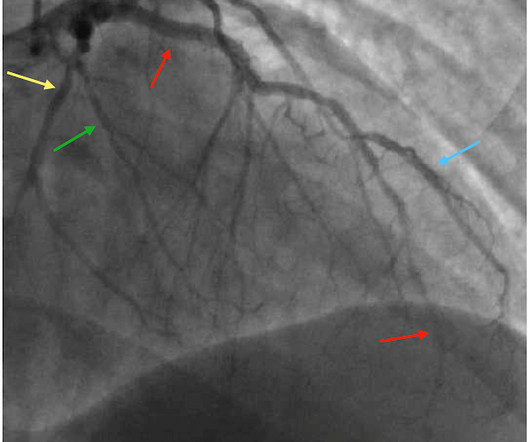
The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1. Available from: [link] If you are wondering about the Barcelona rule, then you should read the above paper by Khawaja et al. Cardiac catheterization occurred around 1pm (18 hours after arrival). 2021;23:187.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content