This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
One study found that the best discrimination of stress cardiomyopathy from ACS was possible with the ratio of NT-proBNP/cTnT on the 2nd day. and an accuracy of ∼96% in detecting stress cardiomyopathy as opposed to ACS. Rallidis Et al. This patient never had ACS. A cut-off value of NT-proBNP/cTnT ratio >7.5
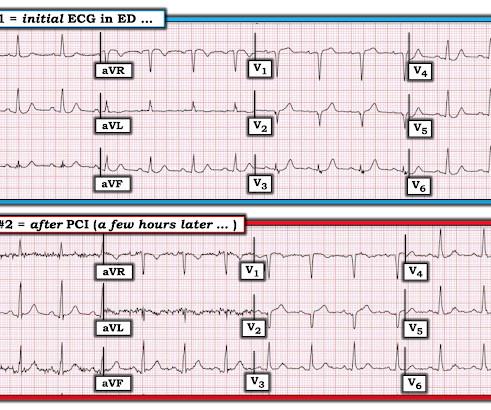
A 41-year-old South Asian male with history of hypertension, alcohol use disorder and hyperlipidemia, who has a strong family history of CAD presented with central substernal burning, pressure, and pain with associated diaphoresis. Transient STEMI was studied by Lemkes et al. Lemkes JS, Janssens GN, van der Hoeven NW, et al.
65 y old male, hypt, IHD, smoker, central chest pain, was in pulm oedema Killip III Great recent article relevant to this: Kosuge M, Ebina T, Hibi K, et al. They show that if there is not >/= 1 mm STE in aVR, then ACS is highly unlikely to be due to severe 3-Vessel disease or Left Main. Am J Cardiol;107(4):495-500.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. A 12 Lead ECG was recorded. 2] Driver, B.
Date: June 30th, 2022 Reference: McGinnis et al. Date: June 30th, 2022 Reference: McGinnis et al. If we thought about ACS, we brought them in. Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. AEM June 2022. AEM June 2022.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. 2021;23:187.
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. link] References 1.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab. Hayakawa A, Tsukahara K, Miyagawa S, et al.
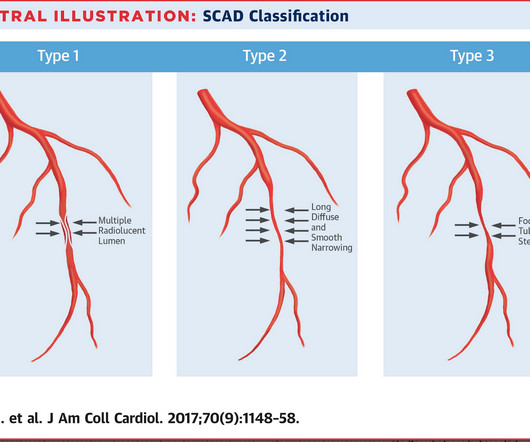
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. Conversely, Matetzky et al.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. I could have told you this (and did tell you this) without an MRI.
Although this is considered a "STEMI equivalent" and the ACC/AHA guidelines even approve of thrombolytics for ACS with this ECG, the usual criteria used to alert the cath lab team of an inbound Code STEMI are not met by this ECG. For instance: sepsis, bleeding, dehydration, hypoxia, and mild ACS. NEJM 362(9):779; March 4, 2009.
He also had non-acute CAD of the RCA (50%) and LCX (50%). CLICK HERE — for a brief article by Rowlands et al that explains these concepts in more detail. Meyers : This ECG was texted to me with no clinical information, and my response was: "That looks like a very subtle LAD OMI. Cath images: Before intervention.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. Smith and Meyers found that patients presenting with high-risk ACS and any ST-depression, even less than 1 mm, maximal in leads V1-V4 to be 97% specific for OMI and 96% specific for OMI requiring emergent PCI. [5] 1] Driver, B. 2] van Gorselen, E.,
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. Widimsky P et al. Knotts et al. This was a 100% acute LM occlusion.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). She also had non-acute CAD of the left main (50%) and LCX (75%). Patel et al., Krucoff et al.) Patel et al. Krucoff et al. Schomig et al. What will you do for this asymptomatic patient??? They opened it.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It is highly associated with proximal LAD occlusion or severe left main ACS and with bad outcomes. See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. This is a very common misread.
I C Glucose-lowering therapy should be considered in ACS patients with glucose levels >10 mmol/L (>180 mg/dL), while episodes of hypoglycaemia (defined as glucose levels <_3.9 I C In patients on metformin and/or SGLT2 inhibitors, renal function should be monitored for at least 3 days after angiography.
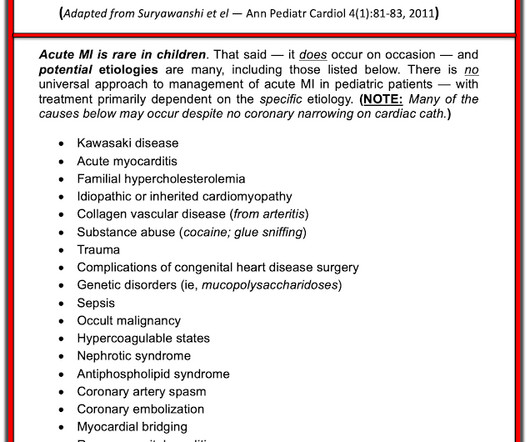
He did have a family history notable for early CAD. A final ECG was perfomed on hospital day 2: Persistent ST elevation in the inferior leads with slight reciprocal ST depression in aVL Teaching points - It is essential to consider ACS in all age groups. He denied drug or alcohol use. ng/mL (ULN 16,000 ng/L, mildly elevated CRP of 8.4
Here are some key features to look out for: CAD & Cardiac Monitor Integration: The application supports integration with cardiac monitors and CAD systems, enhancing your ability to swiftly monitor and respond to patient needs. Integration with ACS to facilitate real-time encounter submissions.
In this study, using risk scores had very little utility Chapman AR, Hesse K, Andrews J, et al. Does a negative ECG and 2 undetectable troponins rule out ACS? Here is an interesting study from Circulation: rnadttir , Pedersen S, Bo Hasselbalch R, et al. Circulation [Internet] 2018;138(16):165465.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content