This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
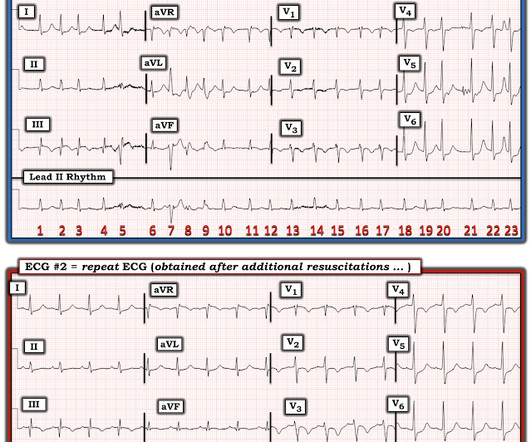
He had a history of CAD with CABG. Does this patient have ACS? Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. He did not have ACS. The remainder were due to other etiologies, (including NonSTEMI ACS).
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. She was defibrillated and resuscitated. Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI.
12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC. In total, he received approximately 40 minutes of CPR and 7 defibrillation attempts. That said, ACS is by far the most common and treatable cause.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). CPR was initiated immediately.
I B ECG monitoring should start immediately and a defibrillator must be ready. I C Glucose-lowering therapy should be considered in ACS patients with glucose levels >10 mmol/L (>180 mg/dL), while episodes of hypoglycaemia (defined as glucose levels <_3.9 STEMI , ST-segment elevation acute myocardial infarction ).
But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation.
Here are some key features to look out for: CAD & Cardiac Monitor Integration: The application supports integration with cardiac monitors and CAD systems, enhancing your ability to swiftly monitor and respond to patient needs. Integration with ACS to facilitate real-time encounter submissions.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content