This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
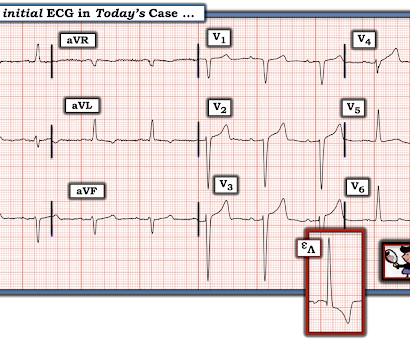
A 41-year-old South Asian male with history of hypertension, alcohol use disorder and hyperlipidemia, who has a strong family history of CAD presented with central substernal burning, pressure, and pain with associated diaphoresis. For clarity in Figure-1 — I've reproduced this 1st ECG in this case that I saw. The rhythm is sinus.
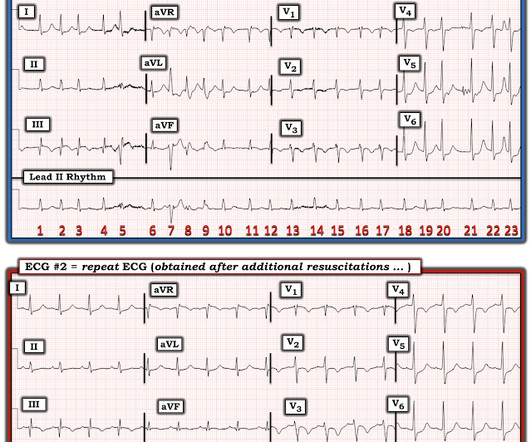
consult: In summary, this is a 47 year old male with past medical history of CAD s/p STEMI in 2010 s/p PCI to LAD with BMS, HTN, tobacco, alcohol and substance abuse that presented with chest pain and found to have ST elevation with T wave inversion in his ECG. He was started on ACS therapy and loaded with Plavix.
ED echo: The left ventricular ejection fraction appears: Severely reduced No pericardial effusion identified. Multivessel CAD 2. Underlying right basilar atelectasis and or infiltrate cannot be excluded. A line predominance, no B lines E-point septal separation 2.24 cm (normal = 0.7 Cardiology consult impression 1.
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. He denied any known history of CAD, but did report ASCVD risk factors to include HTN, HLD, and DM. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain. Background: Chest pain is one of the most common presentations to the ED. In prior decades nearly all patients presenting to EDs with chest pain were admitted to hospital. AEM June 2022.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. Here is the final ECG just prior to ED transfer.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
Was transferred to our ED for emergent PCI, clean cath. Outside ED (no cath lab) 66 yo female with past ho polysubstance use and htn c/o dhest tightness lasting for seconds. Sounds like based on ECGs, cardiologist recommended heparin, no lytics, and transfer to Bend ED. This was sent to me by Susy DeMeester. hs trop 37 ng/L.
He had a history of CAD with CABG. Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Does this patient have ACS? He did not have ACS. The remainder were due to other etiologies, (including NonSTEMI ACS). But approximately 50% were due to non-ACS etiologies.
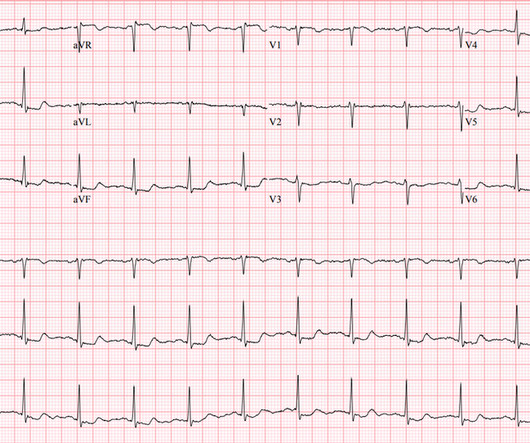
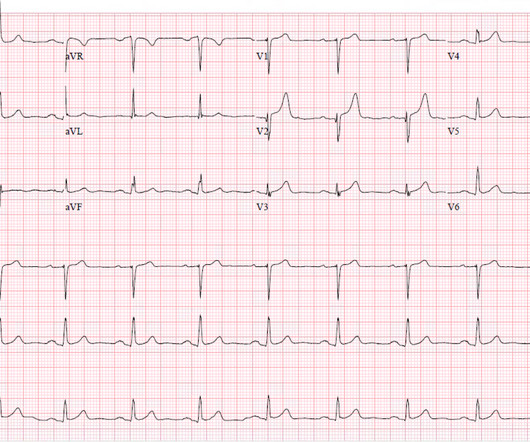
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. Figure-1: The initial ECG that was done in the ED ( See text ).
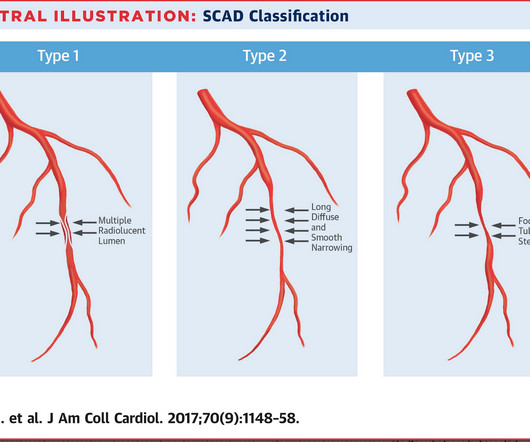
link] A 30 year-old woman was brought to the ED with chest pain. However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. This is written by Brooks Walsh.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Since then, I started looking for OMI EKG findings and not just STEMI. Risk Factors: High Cholesterol.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
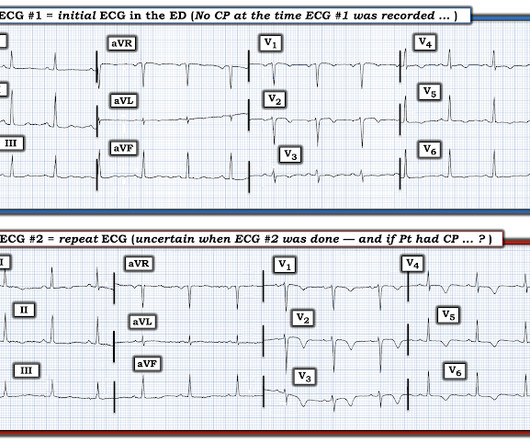
Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. He also had non-acute CAD of the RCA (50%) and LCX (50%). I focus my att ention on the interpretation of the initial ED tracing ( = E CG # 1 in Figure-1 ).
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI. I could have told you this (and did tell you this) without an MRI.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. The cardiologists felt that the ECG did not represent ACS, and thought it was more likely pericarditis, so they did not take him to the cath lab. His first troponin T then resulted elevated at 0.19
She had zero CAD risk factors. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. The 1st “lesson” is, “All bets are off” — when an adult of any age presents to the ED with new-onset chest discomfort. hours of substernal chest pressure.
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. Although this is considered a "STEMI equivalent" and the ACC/AHA guidelines even approve of thrombolytics for ACS with this ECG, the usual criteria used to alert the cath lab team of an inbound Code STEMI are not met by this ECG.
CAD-RADS category 1. --No CT Coronary angiogram is usually used to make ACS much less likely in the context of a patient who is ruled out for acute MI by troponins. Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD
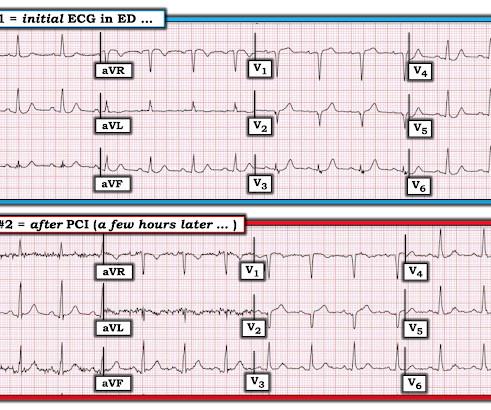
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED. He reported to EMS a medical history of GERD only. However, in this context (i.e.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. Beware crescendo angina in patient with known CAD ST Elevation in aVR Case 7. Only 28% of patients had ACS of any vessel, and, of those patients, the LM was the culprit in just 49% (14% of all cases).(56)
A middle-aged male with h/o CAD and stents presented with typical chest pressure. The patient arrived in the ED and had this ECG recorded: Interpretation? It is highly associated with proximal LAD occlusion or severe left main ACS and with bad outcomes. This is a very common misread. The trick is to find the end of the QRS.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). She was asymptomatic at the time of this ECG recorded on arrival to our ED: What do you think? She also had non-acute CAD of the left main (50%) and LCX (75%). What will you do for this asymptomatic patient??? They opened it.
He did have a family history notable for early CAD. An ECG was perfomed on arrival to our ED: NSR with ST elevation II,III, aVF with reciprocal depression in aVL Would you refer this pediatric patient for emergent PCI? Morrissey and Bracey — regarding consideration of ACS ( A cute C oronary S yndrome ) in a younger patient.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. He was worked up non-emergently in the ED with pain recurring and resolving multiple times during his stay. He had an EKG recorded right away.
But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. The procedure was described as very complex due to severe multivessel CAD, but ultimately PCI was successfully performed to the ostial LCX. Pre-intervention. This idea is erroneous.
Does a negative ECG and 2 undetectable troponins rule out ACS? Conceptually there is a major misunderstanding inherent in the approach by many in the ED. This study looked for death or MI, but 30 day MACE also includes PCI! Many patients do not fit the protocol. Example: Initial trop 10 ng/L and delta of 5 ng/L.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content