This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
One study found that the best discrimination of stress cardiomyopathy from ACS was possible with the ratio of NT-proBNP/cTnT on the 2nd day. and an accuracy of ∼96% in detecting stress cardiomyopathy as opposed to ACS. NT-proBNP and CTnT in ACS and Takotsubo) Smith : However, this is not of any help with the acute diagnosis!
A 41-year-old South Asian male with history of hypertension, alcohol use disorder and hyperlipidemia, who has a strong family history of CAD presented with central substernal burning, pressure, and pain with associated diaphoresis. Patient initially presented at 9 PM to a referring facility with hsTnI 13 (ref: < 34 ng/L) then 30, then 60.
They show that if there is not >/= 1 mm STE in aVR, then ACS is highly unlikely to be due to severe 3-Vessel disease or Left Main. Because if such severe CAD is present, the patient is likely to need CABG. Am J Cardiol;107(4):495-500. why is this important?
Multivessel CAD 2. Suspect type 2 NSTEMI, although difficult to rule out type 1 Given lack of ACS symptoms and multivessel coronary artery disease, her cause was paused for consideration of a heart team approach with consideration for CABG. Underlying right basilar atelectasis and or infiltrate cannot be excluded. cm (normal = 0.7
2. Coronary angiography reveals significant and severe CAD involving all three epicardial vessels. Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). He awoke earlier that morning in his usual state of health. He was taken to the Cath Lab.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? Edited by Smith He also sent me this great case.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. A 12 Lead ECG was recorded.
The bottom line from that episode was that the HEART Pathway appears to have the potential to safely decrease objective cardiac testing, increase early discharge rates and cut median length of stay in low-risk chest pain patients presenting to the ED with suspicion of ACS. If we thought about ACS, we brought them in. AEM June 2022.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chest pain associated with nausea/vomiting 30 min PTA. This was stented with a 2.25
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. Smith : This is ACS even if the troponin returns normal, and the first troponin especially might return normal. This results in Type I MI. This results in Type II MI. Severe HTN d.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chest pain. ACS then becomes less likely. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. How would you assess this ECG? How confident are you in your assessment?
The cardiologist was skeptical of ACS according to his note. Transferred to our ED and taken to cath lab Cath- mild nonobstructive CAD, mild mid LAD bridge Echo- EF 65-70%, normal wall motion, no diastolic dysfunction. Also, just because the angiogram is “negative“, does not mean it is not ACS or OMI. What were the troponins?
He had a history of CAD with CABG. Does this patient have ACS? He did not have ACS. The remainder were due to other etiologies, (including NonSTEMI ACS). But approximately 50% were due to non-ACS etiologies. A middle-aged male had a V Fib arrest. There is profound ST depression especially in I, II, V2-V6.
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. 1] European guidelines add "regardless of biomarkers".
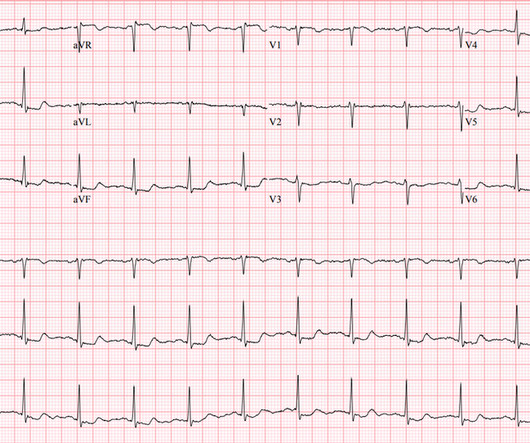
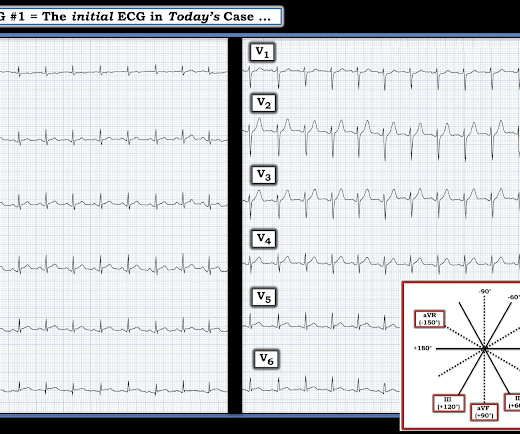
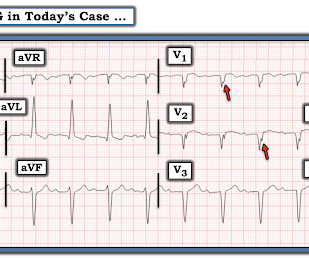
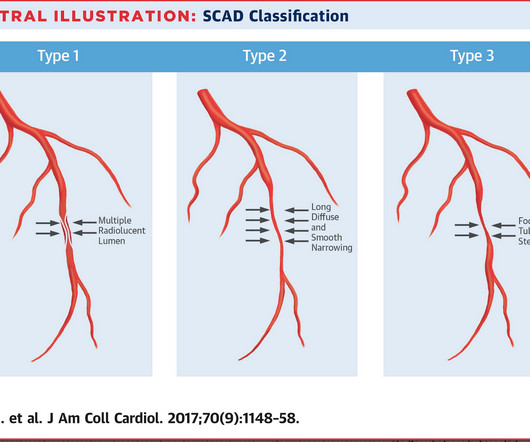
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab. He was diagnosed as NSTEMI.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
No known risk factors for ACS/CAD. The patient was then transferred and admitted for emergent angiogram, however I'm told the cardiologist wasn't quite "convinced" it was ACS/Wellen's. A medic sent this case A 33 yom who presented to an urgent care facility with a complaint of chest pain for several days.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS.
Well, most commonly we’re going to see ACS. As the pregnant population continues to age and with RF and smoking and DM still common we can expect to see pregnant woman with CAD. Improved care of complex. Read More » Welcome back to the tasty morsels of critical care podcast. What can we expect to see in terms of cardiac disease?
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI. V1 has 0.5 mm of elevation. ng/mL [IQR: 0.46, 2.35].
But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. It is proven better than angiography alone in stable angina , and also has been shown to improve decisions on stenting non-culprit lesions in ACS. We need to do some more investigation.
She had zero CAD risk factors. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. hours of substernal chest pressure. It was non-radiating and without other associated symptoms except for nausea. Here was her ECG at time zero: What do you think?
Although this is considered a "STEMI equivalent" and the ACC/AHA guidelines even approve of thrombolytics for ACS with this ECG, the usual criteria used to alert the cath lab team of an inbound Code STEMI are not met by this ECG. 2 The astute paramedic recognized this possibility and announced a CODE STEMI.
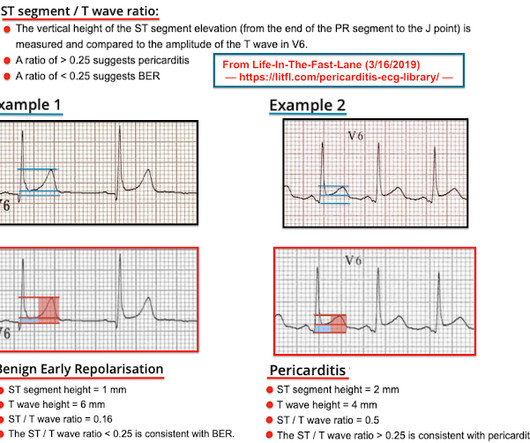
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chest pain. The cardiologists felt that the ECG did not represent ACS, and thought it was more likely pericarditis, so they did not take him to the cath lab. Here is his triage ECG: What do you think? No acute culprit.
He also had non-acute CAD of the RCA (50%) and LCX (50%). Meyers : This ECG was texted to me with no clinical information, and my response was: "That looks like a very subtle LAD OMI. Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes.
CAD-RADS category 1. --No CT Coronary angiogram is usually used to make ACS much less likely in the context of a patient who is ruled out for acute MI by troponins. A repeat troponin returned at 0.45 ng/mL, consistent with reperfused OMI, or Non-OMI. Now, with elevated troponins, Wellens' syndrome is likely.
The patient was transferred immediately for angiogram which revealed no significant CAD, and no intervention was performed. Learning Points: The myocardium doesn't know the etiology of OMI (ACS, spasm, dissection, embolus, etc.), Learning Points: The myocardium doesn't know the etiology of OMI (ACS, spasm, dissection, embolus, etc.),
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. Smith and Meyers found that patients presenting with high-risk ACS and any ST-depression, even less than 1 mm, maximal in leads V1-V4 to be 97% specific for OMI and 96% specific for OMI requiring emergent PCI. [5] He left AMA and is lost to follow-up.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. This case represents the same physiologic event as OMI in terms of the result on the myocardium, therefore with identical ECG features, however there may not be ACS! Clear lungs.
If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. Total LM occlusion can present with STE or STD in aVR. D1 ( STE I, aVL, V5, V6 ) and 2b.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It is highly associated with proximal LAD occlusion or severe left main ACS and with bad outcomes. Here is his ECG: The resident was alarmed at the "ST elevation in III with reciprocal ST depression in aVL" Are you alarmed? This is a very common misread.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). She also had non-acute CAD of the left main (50%) and LCX (75%). By the time the patient arrived at our facility, she had received aspirin and nitroglycerin, and her pain had apparently completely resolved. They opened it. Patel et al.,
I C Blood samples Management Recommendation Level of evidence Serum biomarkers of myocardial infarction ( troponin ) should be sampled as early as possible without delaying reperfusion therapy. I C Symptom relief Symptom Management Recommendation Level of evidence Hypoxia Oxygen is indicated if SaO2 < 90% or PaO2 < 60 mmHg.
He did have a family history notable for early CAD. A final ECG was perfomed on hospital day 2: Persistent ST elevation in the inferior leads with slight reciprocal ST depression in aVL Teaching points - It is essential to consider ACS in all age groups. He denied drug or alcohol use.
Negative trops and negative angiogram does not rule out coronary ischemia or ACS. It is a judgment call retrospectively, but to assume there is no ACS at presentation is very risky, especially in a patient with previously diagnosed severe CAD and poor LV function. It must be diagnosed with IVUS or Optical Coherence Tomography.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. html ) Despite an undetectable troponin and three normal EKGs, the nature of the patients symptoms and his positive cardiac history warranted concern for ACS.
But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. The procedure was described as very complex due to severe multivessel CAD, but ultimately PCI was successfully performed to the ostial LCX. Pre-intervention. This idea is erroneous.
Here are some key features to look out for: CAD & Cardiac Monitor Integration: The application supports integration with cardiac monitors and CAD systems, enhancing your ability to swiftly monitor and respond to patient needs.
Does a negative ECG and 2 undetectable troponins rule out ACS? Available from: [link] --Non-ischemic ECG --Symptoms 3 hours to blood draw AND initial hs-cTnI 5 ng/L or --Any duration of pain and inital value URL (16 ng/L, women, 34 ng/L men) and 3 hour delta 3 ng/L. Identified 65% as low risk for death/MI at 30 days, with 99.7%
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content