This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
They started CPR. Then assume there is ACS. Therefore — recognition of DSI on ECG should prompt consideration of 2 Categories of diagnostic entities : Severe Coronary Disease ( due to LMain, proximal LAD, and/or severe 2- or 3-vessel disease ) — which in the right clinical context may indicate ACS ( A cute C oronary S yndrome ).
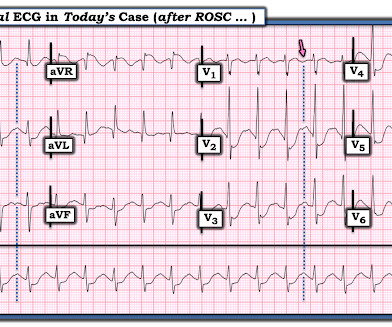
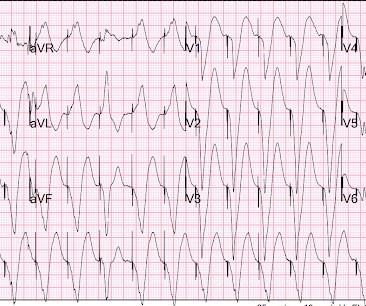
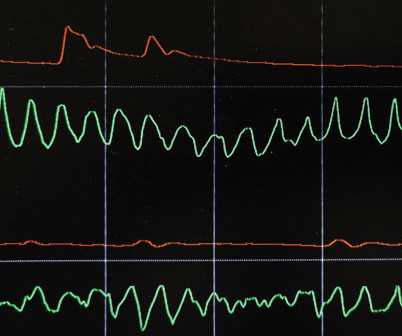
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. EMS arrives and finds the patient in monomorphic ventricular tachycardic (VT) cardiac arrest.
There was no bystander CPR. I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiac arrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? An elderly man collapsed. Medics found him in ventricular fibrillation. So we should activate the cath lab, right?
For patients with OHCA, use of steroids during CPR is of uncertain benefit. Extracorporeal CPR Use of ECPR for patients with cardiac arrest refractory to standard ACLS is reasonable in select patients when provided within an appropriately trained and equipped system of care. COR 2b, LOE B-R. COR 2b, LOE C-LD. COR 2a, LOE B-R.
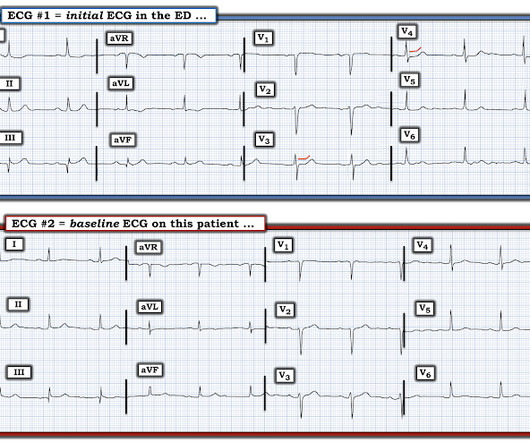
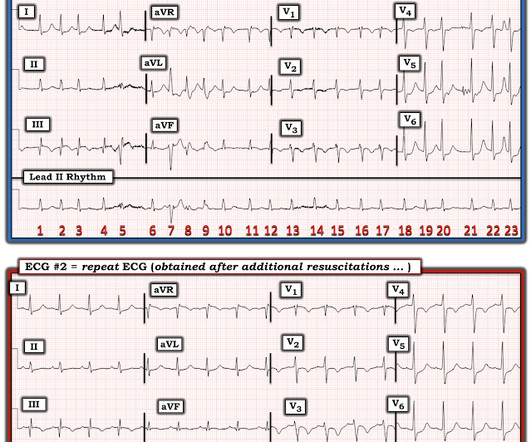
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Here is an article I wrote: Updates on the ECG in ACS. Was this: 1) ACS with ischemia and spontaneous reperfusion? The following 12-lead ECG was recorded at 11 minutes after ROSC.
He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. Therefore, even with a normal or non-diagnostic ECG, a 50 year old male patient should undergo serial ECGs and troponins and be admitted to a monitored bed until MI or ACS can be ruled out. See explanation below.
Assessing the Severity The severity of an electrical burn depends on several factors: the type of current (AC or DC), voltage, the pathway of the current through the body, the duration of contact, and the victim’s overall health. If the victim is unresponsive, CPR is initiated immediately.
1 Overall, survival is poor following cardiac arrest, and is affected by factors including age, comorbidities, witnessed arrest, early CPR, early defibrillation, and return of spontaneous circulation (ROSC). Emmerson AC, Whitbread M, Fothergill RT. Canadian Journal of Emergency Medicine. 20(S1):S67. Resuscitation. 2017;117:97-101.
Data that do not establish neurological risk stratification in the first 6 hours after CA include the patient’s age, duration of CPR, seizure activity, serum lactate level or pH, Glasgow motor subscore in patients who received NMB or sedation, pupillary function in patients who received atropine, and optic nerve sheath diameter (95.3%, 20/21).
He underwent CPR and then was shocked out of VF. ST depression maximal in V1-V4, in the context of ACS symptoms and unexplained by QRS abnormality or tachydysrhythmia, should be considered posterior OMI until proven otherwise. His initial troponin T was 15 ng/L (only two hours since pain onset).
In total, he received approximately 40 minutes of CPR and 7 defibrillation attempts. Learning Points: The myocardium doesn't know the etiology of OMI (ACS, spasm, dissection, embolus, etc.), That said, ACS is by far the most common and treatable cause.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. PMID: 23102885 Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. Clin Exp Emerg Med 2023. JACC Cardiovasc Interv 2018.
This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI. 3-vessel disease can make resuscitation very difficult, since CPR does not perfuse diseased vessels as well as one would like. In aVF it is "coved" (upwardly convex). There is ischemic ST depression in V4-V6.
Reviewed by: Roberto Segura and Mel Ranaweera Article 3: Does hand position affect CPR quality in young children? The effect of hand position on chest compression quality during CPR in young children: Findings from the Videography in Pediatric Resuscitation (VIPER) collaborative. Garabon JJW, Gunz AC, Ali A, Lim R.
This is supplied via alternating current (AC), increasing the risk of titanic contraction of skeletal muscle, leading to kids holding on to the electrical power source. Prolonged CPR should be considered as outcomes are generally good, even if asystole is the presenting rhythm. AC and DC shocks may result in different injury patterns.
CPR was initiated immediately. If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Thursday, November 27, 2014 A patient with chest pain. LV Aneurysm?
A man in his 40s with chest pain and T wave inversion Written by Pendell Meyers Which ACS had more myocardial damage? Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. In syncope, what ar. Acute aphasia.
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
5199481 multidrug OD resp arrest with PEA narrow complex arrest ROSC Brugada pattern suggests cocaine Drug screen: cocaine, fentanyl, meth Posted by Steve Smith at 2:41 PM Email This BlogThis! Laura Case 2468201 V fib ROSC EKG looks like WPW. ROSC from drug overdose arrest, what is the likely.
Simple ACS? Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Repost this one A 30-something with 8 hours of chest pain and an e. A 30-something with It is not a STEMI; it is an opportunity to save my.
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. They will add up in varying magnitudes resulting in a variety of ECG presentations.
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Sunday, August 25, 2013 Anterior ST Elevation - Is it STEMI?
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Tuesday, September 16, 2014 RVH mimicking MI this is from JAMA Internal Medicine: (..)
Optimally, bystander CPR, including the administration of rescue breaths, should be initiated prior to arrival of emergency medical services. References Webb AC, Wheeler A, Ricci A, et al. Every effort should be made to restore adequate oxygenation, ventilation, and perfusion as soon as possible. South Med J. 2021;114(5):266-270.
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them.
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
Simple ACS? Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Repost this one A 30-something with 8 hours of chest pain and an e. A 30-something with It is not a STEMI; it is an opportunity to save my.
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Tuesday, September 17, 2024 Clay Garthe case. Clay Garthe case.
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Thursday, September 8, 2016 Mustafa Alway sept 8 WPW???
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. .
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Friday, October 30, 2020 Maros case of v fib arrest with prehospital RBBB inf (..)
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Sunday, February 4, 2024 Chest pain for one week of and on.
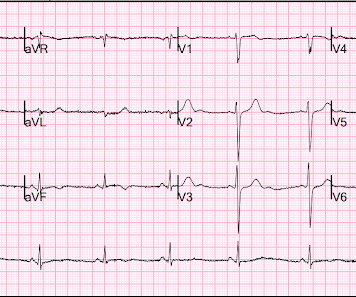
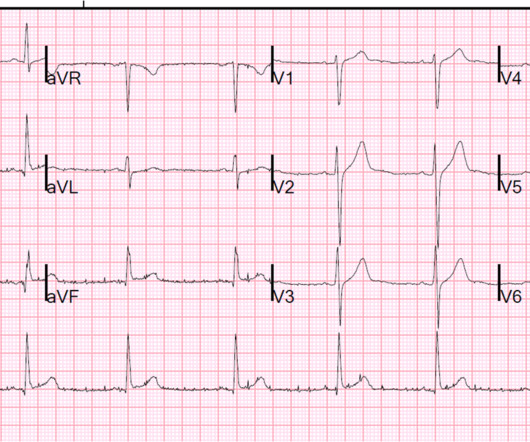
It is highly associated with proximal LAD occlusion or severe left main ACS and with bad outcomes. Here you can see abnormal (diagnostic) ST elevation and an upright T-wave in V2-V3, with diagnostic ST elevation in V4-V6 and in I and aVL, and with reciprocal ST depression in III and aVF. So this is diagnostic of proximal LAD occlusion.
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Wednesday, June 19, 2019 Early Repol changes month to month all trops neg < (..)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content