This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
4,5 Of particular concern is the Sudanese conflict, which began in April 2023, and which has caused the largest internal displacement of a population in documented history. link] Hummell AC, Cummings M. About three-quarters of the countries in sub-Saharan Africa serve as origin or destination points for refugees. 2022;37(1):41-49.
.” Leveraging the ESO Patient Registry During an American College of Surg eons S ite Survey, presented by Matthew Derkrikorian, Trauma Program Manager at Rady Children’s Hospital, offered a look at how Rady Childrens Hospital prepared for and completed the first ACS Site Survey using ESOs updated registry. shared key takeaways.
Causes: ACS, arrhythmia, valvular dysfunction, infection, nonadherence to meds, myocarditis, volume overload. A consensus document from the society for academic emergency medicine/heart failure society of America acute heart failure working group. What are the key tests? Tests: ECG , labs, chest imaging. Erratum in: Ann Emerg Med.
When seeing a South Asian patient with chest pain, concern for ACS must be heightened, given their disproportionately higher risk of CAD, despite often lacking traditional risk factors.) At time of cardiology evaluation, patient was chest pain free, according to documentation.
Most medical documentation is polluted with it, for want of using the persons actual name. The trauma team gathers, the patient is fully awake, listening, wondering what happened to them with a good amount of apprehension and fear. A few simple words by way of update can make all the difference.
Background document for the food advisory committee: certified color additives in food and possible association with attention deficit hyperactivity disorder in children. Scientific Opinion on the re‐evaluation of Allura Red AC (E 129) as a food additive. Refined exposure assessment for Allura Red AC (E 129). 2017): 524-548.
We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. Strictly speaking — this case does not at this time qualify as MINOCA — because the negative cath and 2 normal hs-troponins done 6 hours apart failed to document infarction. (
Sponsor Freed is an AI scribe that listens, transcribes, and writes medical documentation for you. It turns clinicians’ patient conversations into accurate documentation – instantly. Due to system constraints, VCU Health Continuing Education cannot offer subscription services at this time but hopes to do so in the future.
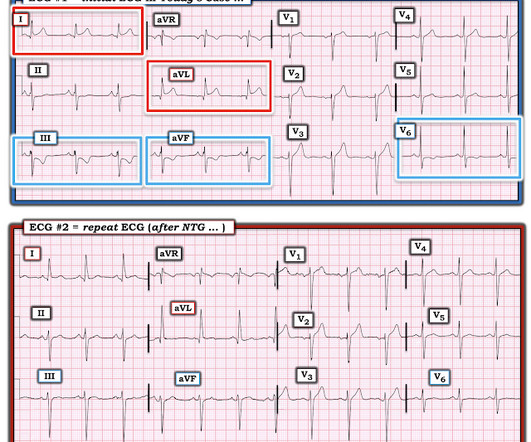
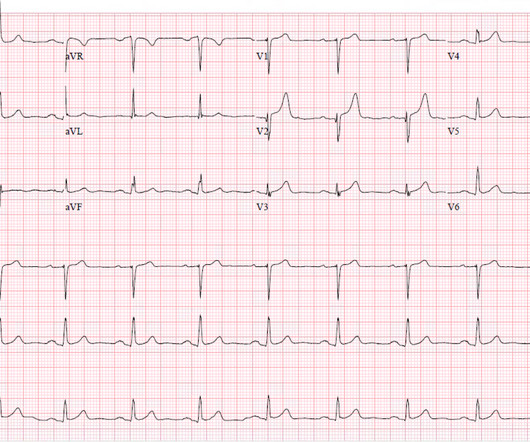
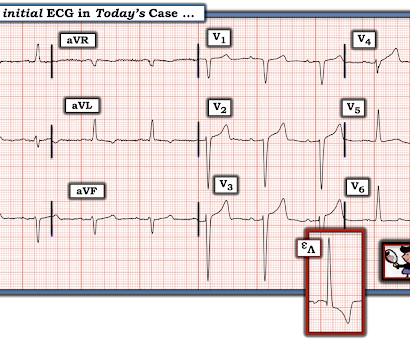
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. The following ECG was obtained. ECG 1 What do you think? of the time.
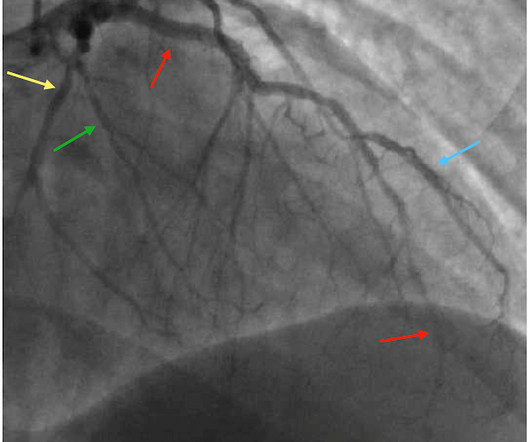
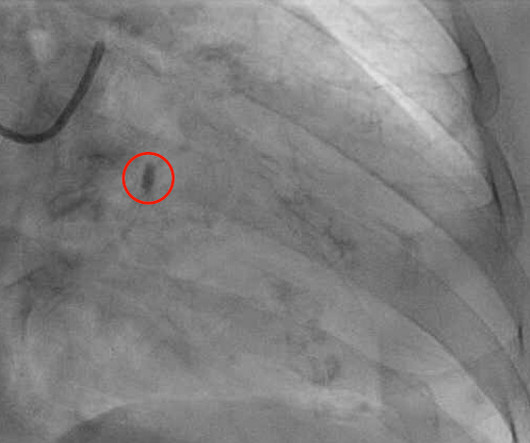
Cardiology documents their interpretation of ECG in their consult note - “atrial paced with old LBBB” The patient stayed at outside hospital (which does not have cardiac cath capabilities). The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1.
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). Repeat cTnI drawn at around 8 AM was 3.910 ng/mL.
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Repeat trop 150 ng/L.
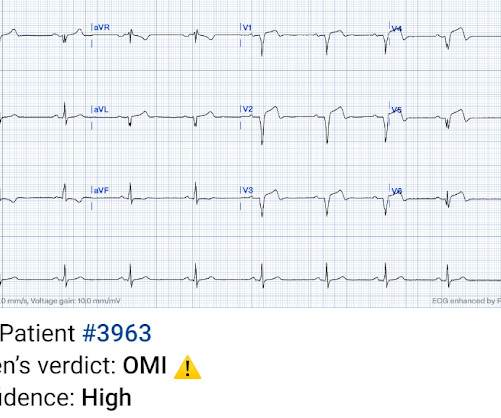
Click here to sign up for Queen of Hearts Access Given the lack of intracranial hemorrhage, the patient was administered aspirin for suspected ACS and cardiology was consulted. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!) Both highly negative. ng/mL and 0.10
Assessing the Severity The severity of an electrical burn depends on several factors: the type of current (AC or DC), voltage, the pathway of the current through the body, the duration of contact, and the victim’s overall health. As EMTs, we’re always prepared to address these life-threatening complications alongside the burns.
While one may argue that nitro really has no mortality benefit in ACS, I have seen patients with CHF present with hyper tension and inferior S-T elevation, in which the providers were scared to even look at the bottle of nitro. References Kimbrell J, Kreinbrook J, Poke D, Kalosza B, Geldner J, Shekhar AC, Miele A, Bouthillet T, Vega J.
None of the patients were documented to have joint disease at follow up. References: Ross RK, Kinlaw AC, Herzog MM, Funk MJ, Gerber JS. There were 2523 children included. Number of adverse effects was similar between the groups, however in the Levofloxacin group 85% of MSK complaints were arthralgias. Pediatrics. 147(6):e202003316.
It is worth doing and documenting serial abdomen exams in non-specific abdo pains. References Meltzer AC, Baumann BM, Chen EH, Shofer FS, Mills AM. d/w Surgical in-patient teams for possible admission for observation rather than directly jumping to imaging.
ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties. ACS surgeons would have sent 6/43 patients for ERCP or MRCP (14%), whereas surgical oncologists would have sent a higher percentage of patients for ERCP or MRCP (7/18 or 38.9%).
The AHA/ACC guidelines recommend emergent cardiac catheterization for patients with concern for ACS and refractory chest pain despite maximum medical therapy defined as aspirin + clopidogrel/ticagrelor + heparin/enoxaparin. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS.
Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. This segues relatively nicely into a section of the document on palliative care. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. To start with there are apparently 5 types of cardiorenal syndrome.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. In either case, prompt cardioversion is indicated.
Some providers were worried about ACS because of this ECG. My answer alleviated their concern for ACS and no further workup was done for ACS. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. Kosuge et al.
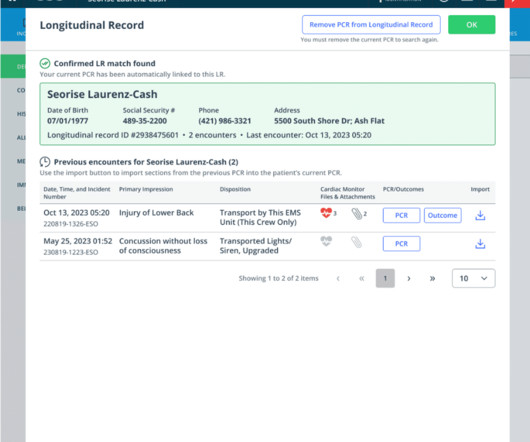
This new feature breaks down the data silos that are inherent in typical prehospital documentation and changes the paradigm of patient care documentation from encounter-based to patient-centric. You’ll now have a holistic view of frequent patients, along with the ability to view previous 12-leads, PCRs and HDE Outcomes.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. The operator documented thoughtful consideration of risks and benefits of stent placement. Initial hscTnI was 10 ng/L (ref. <14).
It is easy to say this in retrospect, especially not being the one in charge of this overcrowded waiting room full of unseen patients, but an elderly patient with known CAD and ongoing ACS-sounding chest pain despite medical management with positive troponin is already an indication for emergent cath, regardless of the ECG!
He had no symptoms of ACS. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." A troponin this high in a patient with no known chronic troponin elevation, and active acute ACS symptoms, has a very high likelihood of type 1 ACS regardless of the ECG.
But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS. But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI.
If it is maximal in V1-V4, and the patient's presentation in consistent with ACS (as this certainly is), then it is DIAGNOSTIC of Occlusion with 90% specificity (We have an upcoming article that proves this). Angiogram: "ACS - Non ST Elevation Myocardial Infarction. This was not recognized. The patient was started on a nitro drip.
There is a substantial ANZICS document on tracheostomy that forms the structure for this tasty morsel. doi: 10.21037/acs.2018.03.01. Intensivists have embraced the tracheostomy as an ICU procedure. It’s one of the most invasive and one of the riskier procedures we do. Surgical anatomy of the trachea. Ann Cardiothorac Surg.
But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. It is proven better than angiography alone in stable angina , and also has been shown to improve decisions on stenting non-culprit lesions in ACS. It could be acute, though probably is not.
The Eastern Association for the Surgery of Trauma (EAST) , the National Association of EMS Physicians (NAEMSP) , and the American College of Surgeons Committee on Trauma (ACS-COT) all support the recommendation against the use of spinal immobilization in patients with isolated penetrating injuries.
I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? But in this case the clinical scenario is not right for acute ACS with OMI, and there is very high voltage, and the patient is very young, (though beware of young patients , even 29 year olds!! There is profound "inferior" ST Depression.
Since ACS is so dynamic, with thrombi forming and lysing continuously, and because the ECG and angiogram are rarely simultaneous, it is probable that de Winter's T-waves are recorded in a window when the artery is barely open. This is the longest lasting I have ever documented a hyperacute T wave without going "up" or "down."
There have been documented cases of overdose, and of note, there is no known antidote. ACS chemical neuroscience molecule spotlight on Contrave. ACS Chem Neurosci. At times, patients may also be taking other diabetes medications such as sulfonylureas or insulin, which could precipitate worsening persistent hypoglycemia.
Hematologic Management Takeaway : They recommend a transfusion threshold < 9 g/dL in those with ACS, but several studies (MINT trial) and guidelines suggest 8 g/dL can be used. Alternatively, a slightly lower PaCO2 within the normal range may be used to maintain a safe pH (>7.2)
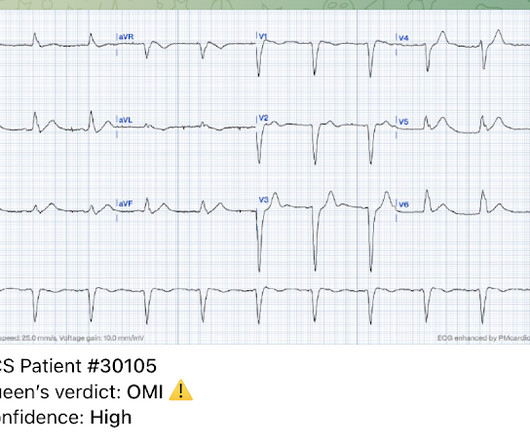
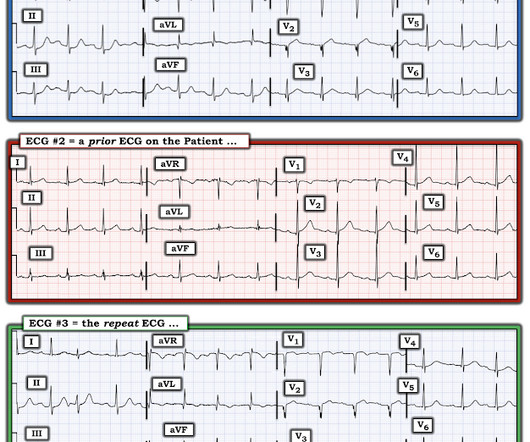
We can see that there is evolution of the elevations, worsening reciprocal change, as well as evolution of posterior involvement (right precordial R-waves with ST depression) There was very little documentation surrounding these ECGs. Beware of ACS presenting with atypical symptoms, including absence of chest pain.
It is true that other documents occasionally describe "abnormal ST segment elevation" in the posterior leads (commonly accepted criteria is 0.5 mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent."
If a patient presents with symptoms of ACS, has an elevated troponin, and has persistent symptoms in spite of medical therapy [antiplatelet, antithrombotic, and anti-ischemic (nitro)], then cath lab activation is indicated regardless of ECG findings. In this case, one might say it is "obvious" MI because of a straight ST segment in aVF.
As he documented, “This patient is experiencing chest pain consistent with an acute coronary syndrome. As cardiology documented, “possible STEMI. Most importantly , while waiting for the paradigm to evolve, maintain focus on our true goal for our patients with ACS: to identify and reperfuse patients with acute occlusion MI.”
This prompted a repeat ECG (we do not have documentation from that time to tell us whether he had persistent, recurrent, or absent pain): Progression of anterior OMI to full Q-wave MI with large pathologic Q-waves in V2-V4 with persistent STE which now meets STEMI criteria (after full thickness infarction/stunning). ng/mL (very elevated).
Diagnosis of acute myocardial infarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads. JACC 2010 Post hoc analysis of the TRITON-TIMI-38 randomized controlled trial comparing prasugrel with clopidogrel among ACS patients undergoing cardiac catheterization.
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al.
Triage documented a complaint of left shoulder pain. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). The ESC states that patients with suspected ACS should go to the cath lab in <2 hours "regardless of ECG or biomarker evidence of MI!!"
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content