This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
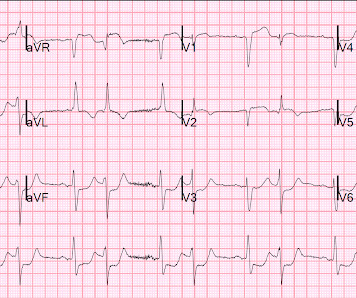
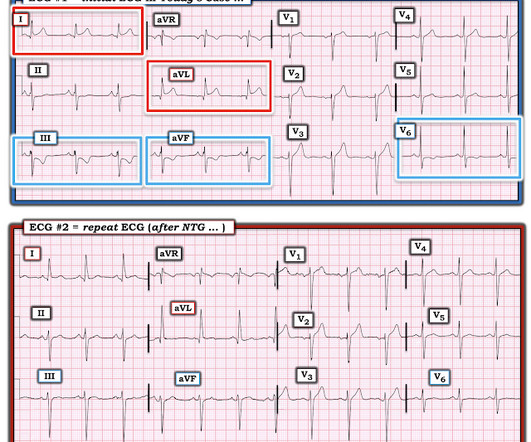
This was written by one of our fine residents, who will soon be an EMS fellow: Michael Perlmutter Case A mid-50s male came to the ED with a burning sensation that was acutely worse while at home. He came to the ED at the urging of his wife. This dynamic change is diagnostic of ACS. ECG at time 82 minutes: What do you think?
Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). In our study, we used COWS alone in the ED, which does utilize restlessness, anxiety, and tachycardia as part of the formula, as the sole evaluation tool for tranq dope withdrawal. Some patients require re-dosing in the ED. 2023 [book].
These findings raise an important question: if the OFC, in its current form, doesnt meaningfully impact outcomes but does extend ED stays, is it time to rethink how (or if) we use it? Clinicians rely on red flags to identify high-risk cases, yet recent research has questioned their effectivenessparticularly in the fast-paced ED setting.
Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. Applicability to Emergency Medicine: For emergency medicine providers, the greatest challenge with this study is that it did not include or account for ED care. Characteristics of sickle cell patients with frequent ED visits and hospitalizations. JAMA Intern Med.
Acute toxic ingestions are a common reason for presentation to the emergency department (ED) and clinical scenarios range from benign accidental ingestions to large overdoses resulting in hemodynamic instability. 13 The treatment of toxic exposures causing hemodynamic instability can represent a unique clinical challenge in the ED.
interesting spontaneous reperfusion case 1413140 prehospital STEMI first ED ECG is here, with 3/10 pain: But this is the same patient just 10 minutes before, with 7/10 pain Isn't it ridiculous to say that the patient has both a STEMI and an NSTEMI? ACS is dynamic. It can't be given one static name. Now the patient has one disease: OMI.
European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED.
A prehospital ECG was similar to the first ED ECG, which is shown below. Here is her initial ED 12-lead ECG: There is atrial fibrillation with a rate of approximately 114. It is most commonly due to demand ischemia, not due to ACS! If it were ACS, what reperfusion options were available? 911 was called. What happened?
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. Labs Laboratory workup in the ED is notable for a leukocytosis of 41,000/L, hemoglobin of 6.5 She is sent to the medical ward after three days in the ED with the diagnoses of resolving septic shock, severe malaria, and AKI.
Blood sampled from existing peripheral IV cannulae yields results equivalent to venepuncture: a systematic review [ 10.1177/2054270419894817 ] Second Line 18 G Should we be placing in the AC? Questions Before Joining (FAQ) Join Now! Future Show: Upping your IV Game Fluids Get dinged for 4, rectal temps on elderly, etc.
May mimic ACS Lesson : 1. By the time she was in the ED, it was no longer massive or submassive, as she had no symptoms, no tachycardia, and normal Echo. And such absence may or may not lead one to pursue other diagnoses. Remember that Pulmonary Embolus: 1. Causes anterior T-wave inversion plus T-wave inversion in III 2.
ED Evaluation: Focus is assessing for other life-threatening treatable conditions: glucose, electrolytes, ECG. Imaging with CT in the ED; MRI while admitted. This is not possible in many EDs. Zehtabchi S, Abdel Baki SG, Malhotra S, Grant AC. If febrile: consider meningitis/encephalitis, perform LP for CSF. Neurocrit Care.
Causes: ACS, arrhythmia, valvular dysfunction, infection, nonadherence to meds, myocarditis, volume overload. ACEP level C recommendation that while there is no specific timing for diuretic therapy, physicians can consider earlier administration of diuretics in ED patients with HF (ACEP). What are the key tests?
25 AC = Anterior chamber, ELISA = enzyme-linked immunosorbent assay, NS = normal saline, PCR = polymerase chain reaction Management Oral Ivermectin 26 150 mcg/kg given once or twice yearly for 10 to 15 years to match the lifespan of the adult worm is the standard treatment. Ramos AN, ed. Bejon P, ed. PLoS Negl Trop Dis.
When seeing a South Asian patient with chest pain, concern for ACS must be heightened, given their disproportionately higher risk of CAD, despite often lacking traditional risk factors.) For clarity in Figure-1 — I've reproduced this 1st ECG in this case that I saw. The rhythm is sinus.
Jarcho JA, ed. 0318502 Lorenzi-Filho G, Genta PR, Figueiredo AC, Inoue D. Longo DL, ed. The patient’s caregivers noticed that the patient had become more short of breath over the last 12 hours and seemed confused. A chest radiograph is obtained, as seen above. Lay Responder Care for an Adult with Out-of-Hospital Cardiac Arrest.
Case: A 32-year-old female presents to the ED with chief complaint of abdominal pain. 10 g/dL in patients with acute coronary syndrome (ACS). Well keep it short, while you keep that EM brain sharp. Her pain started 8 hours ago and became severe within the last 30 minutes. C, and 20 respirations/min.
He was febrile in the ED. Here is the first ED ECG: Sinus tachycardia with deep T-wave inversions in both V1-V6 and in II, III, aVF. male with PMH significant for COPD presented with fever and dyspnea, no chest pain. The patient reported a several day history of difficulty breathing with an associated cough. How did I interpret it?
This is really good Prehospital, ED, and Cardiolog. Fever, tachycardia, hypotension, hypoxia and "SVT" A woman in her 40s with palpitations and chest pre. Flecainide toxicity 4/21/21 2597782 This case was flagged as a false positive cath lab. A man in his 60s with diaphoresis, vomiting, and i.
The syphilis and trichomonas tests come back negative in the ED, but his rapid HIV test is positive. How should clinicians approach the diagnosis and management of HIV in the ED? 11 These cardiovascular complications have further increased ED visits by HIV-positive patients by three times compared to individuals without HIV.
EDACS is broader—captures symptoms suspicious for ACS, not just chest pain, and performs well in low-risk patients. Between 6-9 million patients present to the ED for chest pain annually. Clinical Bottom Line Both HEART and EDACS are best utilized for identifying patients with suspected ACS who are at low risk for MACE.
👉 Click here to access the PERC RULE on MDCalc 👉 Click here to access the Wells’ Criteria on MDCalc 🤕 Case A 35 year old woman with no past medical history presents to the ED with pleuritic chest pain and shortness of breath. She is tachypenic but has a normal heart rate and oxygen saturation.
Ed Dellert, RN, MBA, CAE, FACEHP Chief Executive Officer American Burn Association Stay connected. ABA Strategic Collaborations : The ABA continues to strengthen its role as a convener and collaborator across the burn and broader trauma communities. As we shape the future together, your voice remains at the center. More to come in September.
In the ED, after intubation due to AMS, he was found to be hypotensive and tachycardic to the 160s. He was started on ACS therapy and loaded with Plavix. This procedures were done due to prior similar presentations and concern of ACS. This is the most likely caused of his fixed ST elevation and no concern for ACS.
Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. (4)
Ed Burns (from Life in the Fast Lane) sent me this. See what happens when one fails to diagnose STEMI. Serial ECG recordings are essential: paramedic mak. Are These Wellens' Waves?? (4)
The 88 year old with dementia warehoused in the ED for days — 3 or 4 or 5 — while services battle over who might be bothered to look after them. Or, we can bring you back for an outpatient CT scan tomorrow and see you in the ED after for the results and reassessment. Questions Before Joining (FAQ) Join Now! Their cat.
ED echo: The left ventricular ejection fraction appears: Severely reduced No pericardial effusion identified. Suspect type 2 NSTEMI, although difficult to rule out type 1 Given lack of ACS symptoms and multivessel coronary artery disease, her cause was paused for consideration of a heart team approach with consideration for CABG.
Emergency (ED placement) Transvenous Pacer appears. Back to basics: what is this rhythm? What are your. 30 yo woman with trapezius pain. HEART Pathway =. Good case for showing a flutter and LBBB, Good cas. What is this rhythm? Back to basics. Is there Terminal QRS Distortion? What is so unusual about this inferior OMI (which.
A 20-something woman with Chest Pain Eric Abrams case A woman in her 50s with dyspnea and bradycardia Where is the focus of this tachycardia? Ventricular Fibrillation, ROSC after perfusion res. (4)
Dysnpea and Elevated troponin Takotsubo that looks like LVA Huge Precordial ST Elevation in an ED Patient Tachycardia, hyperthyroid, and ST elevation. Is this just right bundle branch block? Besides the Nonspecific T-wave Inversion in aVL, W.
Chest pain resolved, and a "Normal" ED ECG 2 cases of false pos STE aVL What will you do for this patient transferred to y. 30-something male with confusion, weakness, headac. A Patient with Respiratory Failure and a Computer. Cardiac arrest with STEMI pattern: no acute corona. How accurate are the Monitor leads for ST Elevation?
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Trauma season is at hand and like all other pediatric emergency departments in the country, we find our ED breaking ( pun intended ) at the seams with orthopedic injuries. We see all different flavors of upper extremity injuries. The minority of parents would have wanted clinic follow up (6%) and reimaging (14%). J Bone Joint Surg Br.
In the age of high sensitivity troponins and the HEART pathway, which patients are safe to discharge home from the ED? What are the most useful historical factors to increase and decrease your pretest probability for ACS? Which cardiac risk factors have predictive value for ACS?
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” ACS is usually amongst this differential, as cardiovascular disease is a leading cause of morbidity and mortality in this population. The proportion of patients with ACS at the index visit or within 30 days. *
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
A 5-year-old female presented to the emergency department (ED) with a one-year history of gradually increasing anterior neck swelling. She was discharged from the ED on levothyroxine 25 mcg daily with endocrinology outpatient follow-up. The patient had no significant past medical history. Pediatric neck masses. Pediatr Rev.
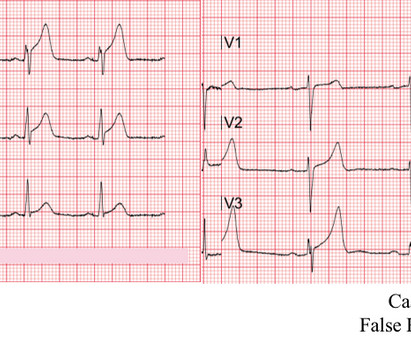
They also discuss the challenges of pulse palpation and the need for more rigorous research in EMS and ED settings. References: Kimbrell J, Kreinbrook J, Poke D, Kalosza B, Geldner J, Shekhar AC, Miele A, Bouthillet T, Vega J. They emphasize the importance of confirming electrical capture before assuming mechanical capture.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. Here is the final ECG just prior to ED transfer. It’s important to stress the presence of a normal QRS (i.e., The pathology is now painfully evident.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content