

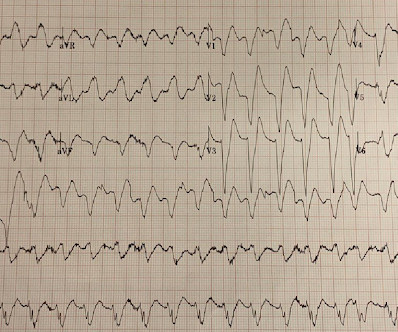
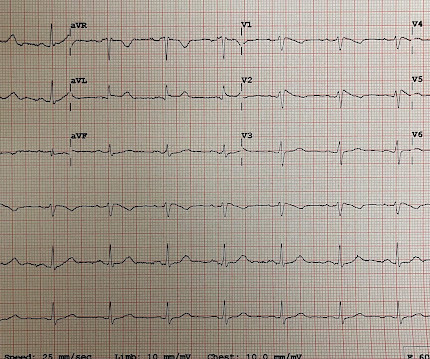
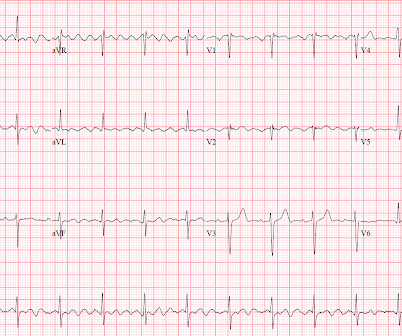
Is this STEMI or NSTEMI? Neither. It is OMI.
Dr. Smith's ECG Blog
MAY 20, 2025
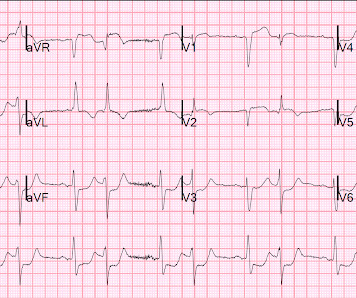
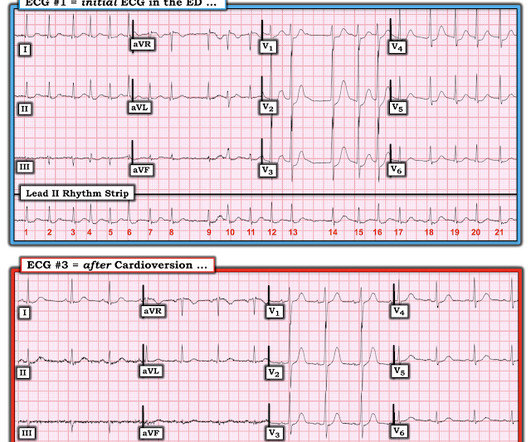
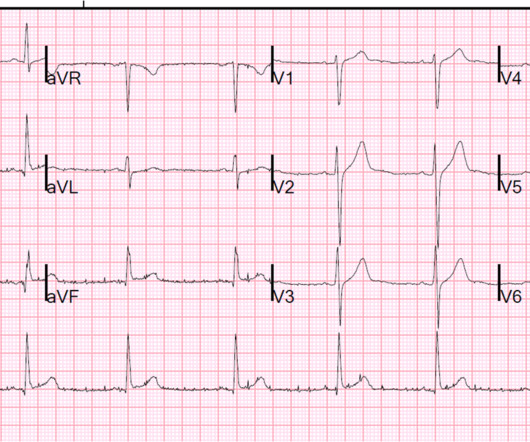
interesting spontaneous reperfusion case 1413140 prehospital STEMI first ED ECG is here, with 3/10 pain: But this is the same patient just 10 minutes before, with 7/10 pain Isn't it ridiculous to say that the patient has both a STEMI and an NSTEMI? ACS is dynamic. It can't be given one static name.


























Let's personalize your content