This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Then we can correct that modified QT for heart rate.
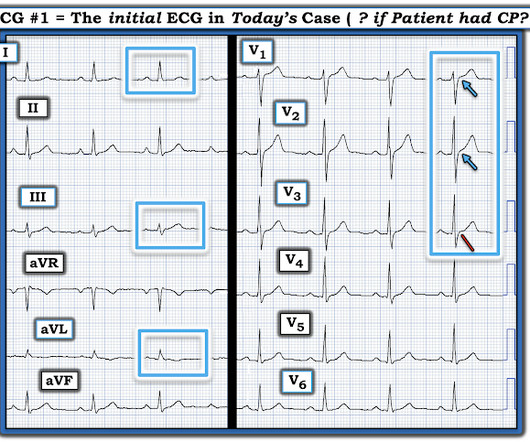
Hershey Medical Center Editors : Alex Blau, DO; Michael DeFilippo, DO, Assistant Professor of EM & EMS, WashU School of Medicine Clinical Case The day after a snowstorm you are working for a rural, advanced life support (ALS) agency and you are called to a 62-year-old gentleman with chest pain. Which hospital do you choose?
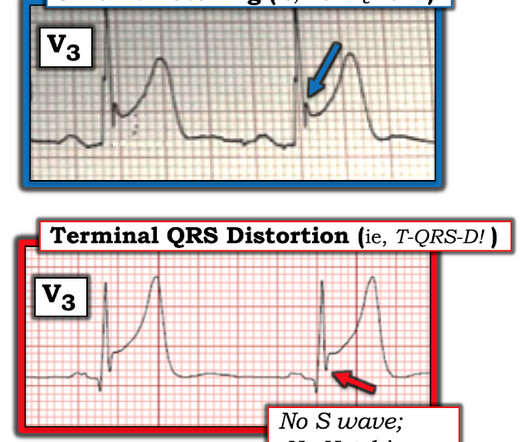
al in 2008, and is eponymously named after the main author. This typically occurs in the setting of a rapidly reperfused coronary artery following a myocardial infarction. The pattern is mostly described with LAD OMI, but has been reported in other coronary distributions as well. The ST-segment in lead V1 has upward convexity.
Does that normal troponin and ECG obviate the need for cardiology consultation for my patient with a concerning story for acute coronary syndrome? Knack SKS, Scott N, Driver BE, Pet al. Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Freund Y, Cachanado M, Aubry A, et al. Penaloza A, Verschuren F, Meyer G, et al.
Perkins ZB, Greenhalgh R, Avest E, et al. Sutori D, Erdelyi LS, Uri I, et al. Dorsett M, Allen H, Garbacz H, et al. Baker PO, Karim SR, Smith SW, et al. Perkins ZB, Greenhalgh R, Avest E, et al. Sutori D, Erdelyi LS, Uri I, et al. Baker PO, Karim SR, Smith SW, et al. 2025;160:432-440 2. 2025 [link] 4.
See this photo of Figure 1 in Wellens' first paper (de Zwann C et al. Had the patient undergone standard angiography, the diagnosis of PE would only be considered because of absence of coronary disease. Just like coronary occlusion, pulm artery occlusion can be transient, and the patient recovers.
A quadruple coronary bypass. Coronary artery disease that had developed over decades. Langtry S, Wild J, et al. And left untreated, it chips away more than just your mind. It takes your body, too. The Hidden Cost In December 2024—long after I’d retired from the field—I underwent open-heart surgery. Was PTSD the sole cause?
See this case in which the ECG which was recorded after stabilization is diagnostic: ST depression, pulmonary edema, and severe hypertension: is this demand ischemia or acute coronary syndrome? Co-culprit is a 85% bifurcating lesion of the large LADD1 related to above LAD lesion This is an important article by Widimsky et al.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chest pain. The most common way is by delivering a lead into the coronary sinus ostium in the RA, which wraps around the posterolateral portion of the LV. Kaye et al.
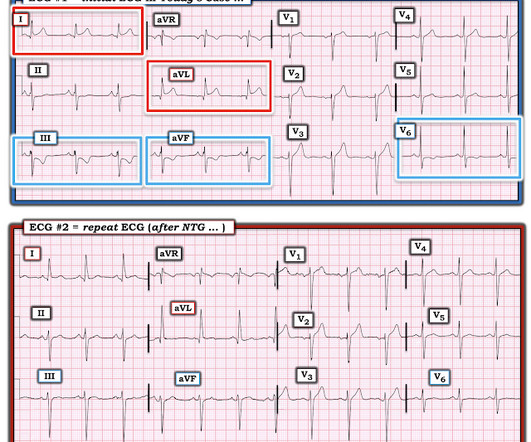
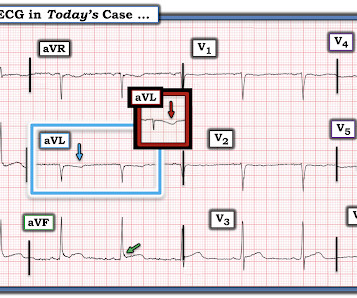
The T wave changes that have occurred are widespread, and not in a typical coronary distribution. Rallidis Et al. Each time the patient underwent cardiac catheterization — and each time, she had patent coronary arteries! Note also the loss of R wave amplitude in ECG #2 compared to ECG #1. This patient never had ACS.
Transient STEMI was studied by Lemkes et al. Lemkes JS, Janssens GN, van der Hoeven NW, et al. Available from: [link] Lemkes et al. Coronary angiography before and after intervention is shown below. This is really a transient OMI (or transient STEMI if one uses that terminology and it has diagnostic ST Elevation).
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI).
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management.
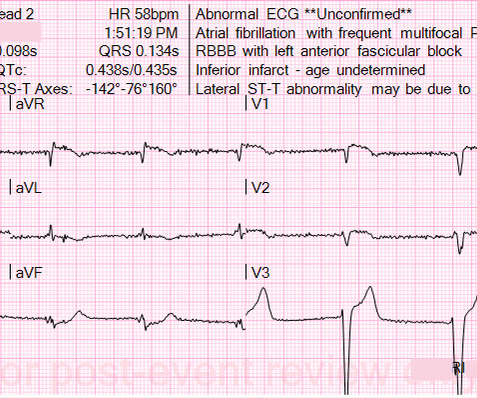
Autolysis and reperfusion the right coronary artery prior to ED presentation was likely responsible for the subtle biphasic terminal T wave inversion seen on his presenting ECG. 12 hours after presentation the right coronary artery likely RE-occluded, manifesting in the clear ST segment elevation myocardial infarction seen at 2:00 AM.
65 y old male, hypt, IHD, smoker, central chest pain, was in pulm oedema Killip III Great recent article relevant to this: Kosuge M, Ebina T, Hibi K, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol;107(4):495-500.
vs 5.1%; RR Feldman E, et al; 2019. vs 5.1%; RR Feldman E, et al; 2019. vs 40.6%; p Desborough M, et al; 2017. vs 40.6%; p Desborough M, et al; 2017. 0.84) Barletta J, et al; 2016. 0.84) Barletta J, et al; 2016. Kapapa T, et al; 2014. Kapapa T, et al; 2014. units; 95% CI 1.16
5 Miller J, et al. Findings: The accelerated protocol did not significantly increase safe discharges (57.8% […] The post Rapid Acute Coronary Syndrome Evaluation Over One Hour With High-Sensitivity Cardiac Troponin I: A United States-Based Stepped-Wedge, Randomized Trial appeared first on EMOttawa Blog. Ann Emerg Med.
The cath lab was activated and the coronaries were normal. Peguero JG et al. Procedure: Coronary angiography. Left heart catheterizatio (the AL-1 catheter entered the left ventricle during attempts at engaging the anomalous RCA). RCA: anomalous take-off probably from the left coronary cusp. Findings: 1.
An 86-year-old man with a history of hypertension, hyperlipidemia, cardiomyopathy, and our-vessel coronary artery bypass five years prior presented to the emergency department (ED) with one hour of sudden-onset retrosternal, pressure-like chest pain radiating to the left arm. The ECG obtained in the ED is shown above.
Date: November 22, 2023 Reference: Stopyra et al. Date: November 22, 2023 Reference: Stopyra et al. A 12-lead electrocardiogram (ECG) demonstrates ST elevations in leads II, III, and aVF with ST depressions in leads I and aVL and the team begins transport to the nearest percutaneous coronary intervention (PCI) capable hospital.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. years, with the interval as long as 12 or 18 years in some studies. Unfortunately, vascular remodeling is variable and inconsistent.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Reference: McGinnis et al.
Why Was Cardiac Cath Negative for Coronary Disease? As noted by Dr. Nossen — this patient qualified as MINOCA ( M yocardial I nfarction with N on- O bstructive C oronary A rteries ) — since troponin was positive on his 2nd admission, yet there was no evidence of obstructive coronary disease on cath.
Methodology: 3/5 Usefulness: 2/5 Ashburn NP, et al. Question and Methods: The authors completed preplanned subgroup analyses to determine if a 0-1 hour ultra-sensitive troponin […] The post Sensitivity Cardiac Troponin T Among Patients With Known Coronary Artery Disease appeared first on EMOttawa Blog. JAMA Cardiol.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. Nikus et al. Kontos et al. Kontos et al. Bischof et al.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. It is spread to V2 and V3. References Naidu, S.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Amsterdam et al. Alencar et al.
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Reference: Wang et al.
One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. Discussion When the QRS is normal, is the encountered ST/T changes that beget suspicion for LAD ACS (as in both of these cases) the result of occlusive coronary thrombus, or simply a normal variant?
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g. potassium) were within normal parameter.
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
Methodology: 3/5 Usefulness: 1/5 Georgiopoulos G, et al. The post Modification of the GRACE Risk Score for Risk Prediction in Patients With Acute Coronary Syndromes appeared first on EMOttawa Blog. JAMA Cardiol. Methods: Retrospective.
[display_podcast] Date: May 16, 2018 Reference: Freund et al. display_podcast] Date: May 16, 2018 Reference: Freund et al. Reference: Freund et al. Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial.
The latest is Langlois-Carbonneau et al. But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! But according to Langlois-Carbonneau et al.,
Extracorporeal membrane oxygenation Of patients with out-of-hospital cardiac arrest presenting to the ED in refractory VF, a majority have significant coronary artery disease, much of which is amenable to percutaneous coronary intervention. References Tsao CW, et al. Benjamin EJ, et al. Kimblad H, et al.
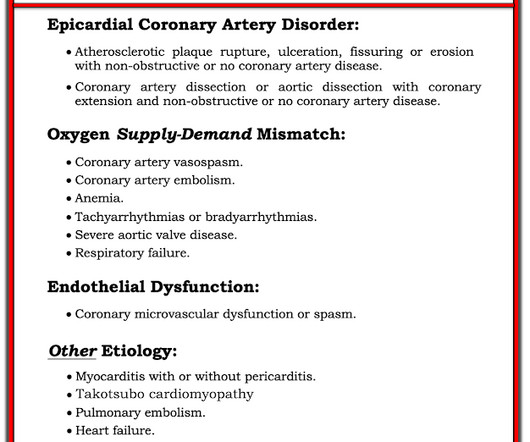
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). link] [1] Zachary et al. Utility of the history and physical examination in the detection of Acute Coronary Syndromes in emergency department patients. Western Journal of Emergency Medicine, 18 (4), 752-760. [2]
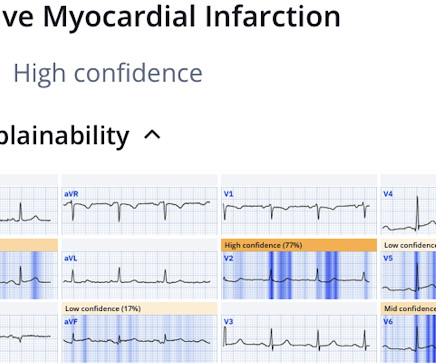
Coronaries were clean. Not OMI with High Confidence Click here to sign up for Queen of Hearts Access We showed that the Queen of Hearts decreases false positive cath lab activations: 1) Published recently in Prehospital Emergency Care Baker PO et al. 2) To be presented at AHA conference in Chicago in 2 weeks: Sharkey SW et al.
It has been said that it can take 17 years for 14% of research to reach the patients’ bedside ( Morris et al 2011 ). Talk I: Knowledge Translation in the Digital Age The first talk was on knowledge translation (KT) in the digital age. A number of examples of the KT problem were provided.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content