This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Skip to content Twitter Google+ Facebook Reddit RSS The Bottom Line A compendium of critical appraisals in Intensive Care Medicine research and related specialties Home About Us Summaries Intensive Care Medicine Emergency Medicine Peri-operative Medicine Blog News EBM Editorial Submit a review Wessex ICS You are here: Home BlogEmergency Evidence Updates (..)
You load him in the back of your ambulance and acquire a 12-lead electrocardiogram (ECG) and it is as follows: You are 5 minutes from a local community hospital and 45 minutes from the tertiary care center with percutaneous coronary intervention (PCI) capabilities. Which hospital do you choose? This speaks to the true essence of the question.
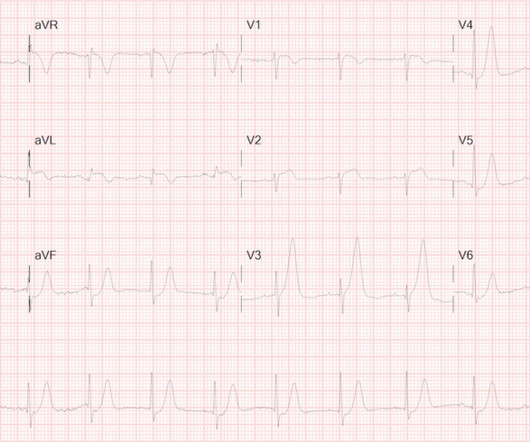
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chest pain. The following ECG was obtained in the emergencydepartment during active chest pain. He said he had had three episodes of chest pain that day while urinating.
Nevertheless, Sunday morning the pain became much worse so he drove himself to the emergencydepartment. His pain is 9/10. 50-something gentleman with three week history of common cold symptoms with persistent coughing.
Written by Jesse McLaren An 80 year old with a history of CHF, ESRD on dialysis, and multiple prior cardiac stents presented to the emergencydepartment with 3 days of intermittent chest pain and shortness of breath that resolved after nitro, which felt like prior episodes of angina. So which was the culprit?
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management.
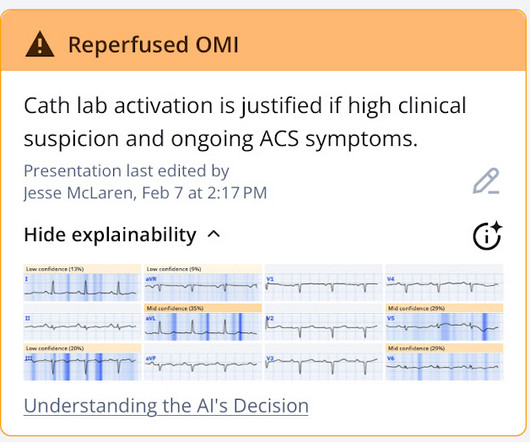
At the time of evaluation in the emergencydepartment he is pain free at which time the following ECG is obtained: The above tracing and clinical vignette were sent to Dr. Smith who responded with the following: “It looks like a reperfused, inferior and lateral OMI.
He is a GP by training but works in EmergencyDepartment, Anaesthesia, Internal Medicine and Paediatrics. He has a wonderful #FOAMed blog and podcast called Broomedocs and also work […] The post SGEM#326: The SALSA Study: Hypertonic Saline to Treat Hyponatremia first appeared on The Skeptics Guide to Emergency Medicine.
But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! See > 50 cases on Dr. Smiths EGC Blog. Am J Emerg Med. Am J Emerg Med.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. Regular readers of this ECG Blog will be well familiar with many of these points. No ECG was ordered on Day #1.
Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. In October 2022, the American College of Cardiology released an updated expert consensus decision regarding the evaluation of chest pain in the emergencydepartment.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. 2014 AHA/ACC guideline for the management of patients with non-ST elevation acute coronary syndromes.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Back to the case. Guagliumi, G.,
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? Emergent cardiac outcomes in patients with normal electrocardiograms in the emergencydepartment. Am J Emerg Med.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Annals of Emergency Medicine 2011; Suppl 58(4): S211.
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Written by Bobby Nicholson What do you think of this “STEMI”? Blood glucose was not low at 162 mg/dL.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). From there you can link to other great websites (including Dr. Smith's ECG Blog) that provide multiple case studies of both subtle and overt hyperkalemia. Western Journal of Emergency Medicine, 18 (4), 752-760. [2]
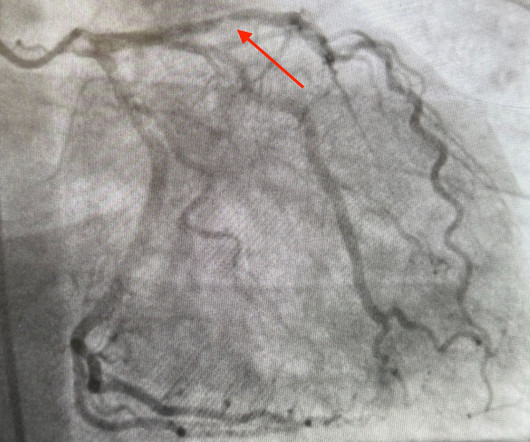
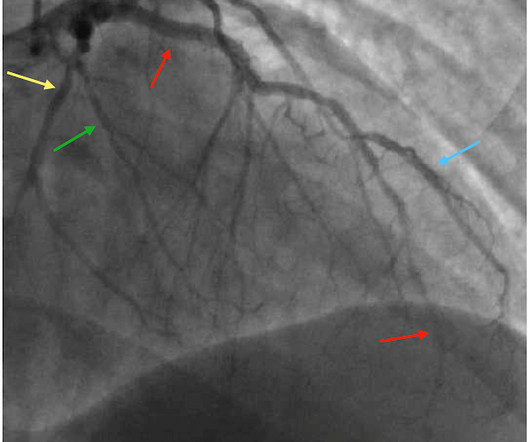
Angiogram: Severe two-vessel coronary artery disease with possible co-culprits (90% proximal circumflex, 70% mid/distal RCA) in the setting of non-ST elevation myocardial infarction. Marked ST depression from multi-vessel coronary disease serves to attentuate what would have been ST elevation in leads II and aVF ).
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
AslangerE A 65-year-old gentleman presented to the emergencydepartment after experiencing two recent ICD shocks in the preceding hours. A recent angiogram report indicated a totally occluded left anterior descending artery (LAD) and right coronary artery (RCA), with 30-40% narrowings in the left circumflex artery (LCx).
She presented to the emergencydepartment after a couple of days of chest discomfort. The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!)
A 50 year old presented to the emergencydepartment of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chest pain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation. The Need for Immediate Transport?
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
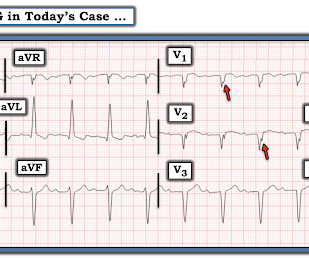
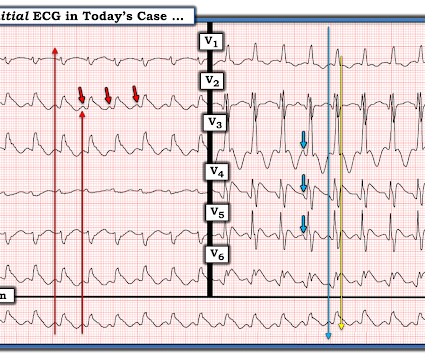
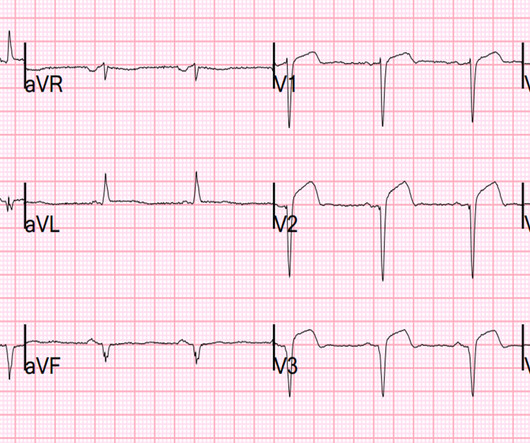
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. But STEMI criteria is only 43% sensitive for OMI.[1] Int J Cardiol 2024 2.
Am J Emerg Med. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. 2022 Jan;51:384-387.
Many systems now refrain from showing computer "normal" ECGs to the busy emergency physicians at triage because of very poorly conceived articles that say that if the computer algorithm says "normal," the emergency physician should not be bothered. We have shown many examples of this on this blog.
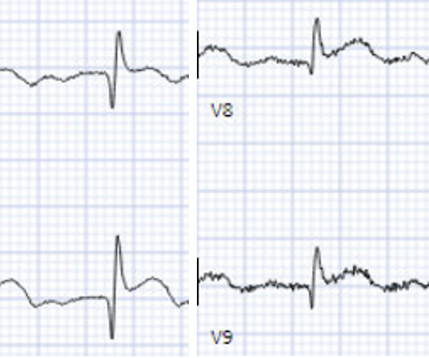
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). link] ] Outcome The patient emerged neurologically intact. Clinical Cardiology 2019.
According to this data a triage ECG labeled ‘normal’ rules out the possibility of acute coronary occlusion. This is obviously unreliable data, as Dr. Smith’s Blog has published 51 cases of OMI with ECGs labeled ‘normal’ , 35 of which were identified by the Queen of Hearts – with 10 examples here. It should never have been published.
Hgb 11g/dL (110g/L) and leukocytosis, and a mildly elevated troponin (36 ng/L, with normal 1mm STE in aVR due to ACS will require coronary artery bypass surgery for revascularization, the infarct artery is often not the LM, but rather the LAD or severe 3-vessel disease. Incidence of an acute coronary occlusion. Left main?
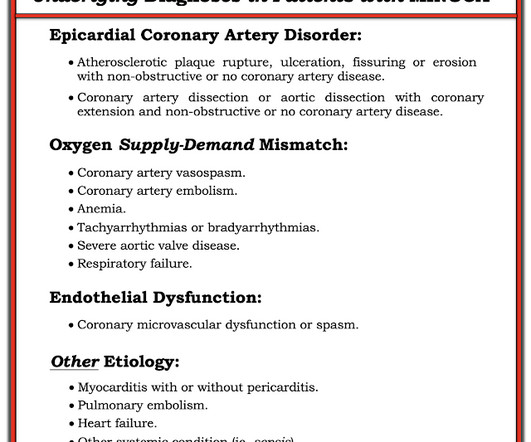
She was unable to be defibrillated but was cannulated and placed on ECMO in our EmergencyDepartment (ECLS - extracorporeal life support). Angiography showed normal coronaries. MINOCA: Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease). 2) overlooked obstructive coronary disease (e.g.,
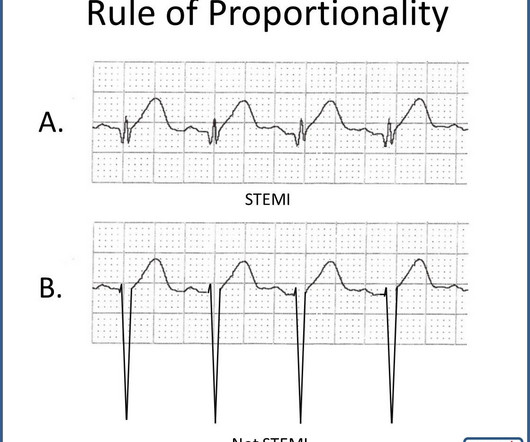
He is transported to the EmergencyDepartment where care is transferred to a nurse. Assuming the patient has signs and symptoms of an acute coronary syndrome (you always want clinical correlation), you should consider the T-waves in example A. Further Reading Take a look at these blog posts from Dr. Smith’s ECG Blog.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
Submitted by anonymous, written by Pendell Meyers A woman in her 50s presented to the EmergencyDepartment with chest pain and shortness of breath that woke her from sleep, with diaphoresis. A very similar case to the one presented today appears in the January 17, 2023 post of Dr. Smith’s ECG Blog.
He arrived in the emergencydepartment hemodynamically stable. The next day, and angiogram showed normal coronary arteries. He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. On his bib it stated that he had a congenital heart disorder. His initial ECG is shown here. He awoke and did well.
Earlier this morning, he developed severe chest pain that lasted about 6-7 hours along with shortness of breath at which point he called 911 and was brought to the emergencydepartment. Cath Lab was activated and patient underwent left heart catheterization coronary angiogram. There is also 1-2 mm ST depression in leads V1-V3.
He presented to the EmergencyDepartment with a blood pressure of 111/66 and a pulse of 117. An angiogram showed no acute coronary lesions. This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chest pain.
It was ongoing on arrival in the emergencydepartment. STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. Am J Emerg Med 2023 2. What do you think?
difficult to see due to corneal edema) EmergencyDepartment Management All patients should get emergency ophthalmologic consultation Start with eye drops (see table below) and add systemic medications if severe or refractory symptoms/IOP. Decreased visual acuity, Cup to disc ratio >0.6 Cup to disc ratio >0.6
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. It is not a missed STEMI, but it is a missed coronary occlusion. Ann Emerg Med 1998;31(1):3-11.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Relationship between an in-farct related artery, acute total coronary occlusion, and mortality in patients with ST-segment and non-ST-segment myocardial infarction.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
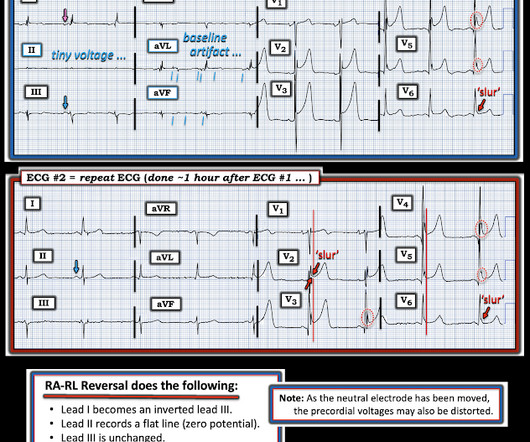
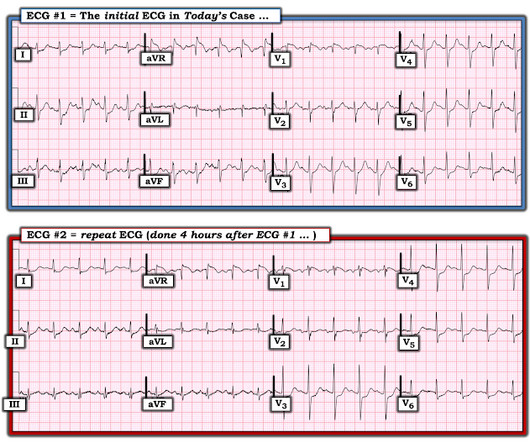
The pain resolved as he arrived to the emergencydepartment. As has been emphasized on numerous blog posts on this site — more than a single tracing will usually be needed for optimal diagnosis whenever the slightest of doubt regarding acuity exists. He had 2 episodes over the past 2 days of similar chest tightness.
A prospective validation of the HEART score for chest pain patients at the emergencydepartment. External validation of the emergencydepartment assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP). Am J Emerg Med 2020 3. Backus BE, Six AJ, Kelder JC, et al. Int J Cardiol 2013 2. Lancet 2015 6.
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content