

Interns are not (yet) poisoned by the STEMI/NSTEMI paradigm
Dr. Smith's ECG Blog
JUNE 10, 2025
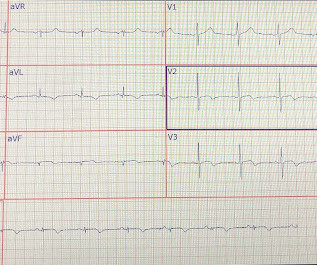
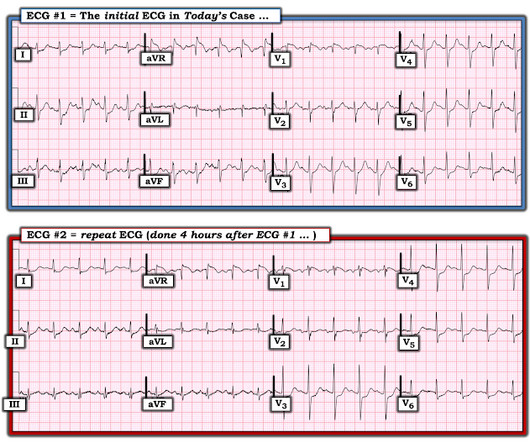
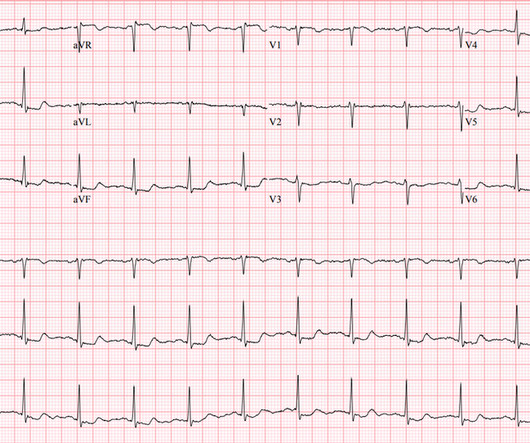
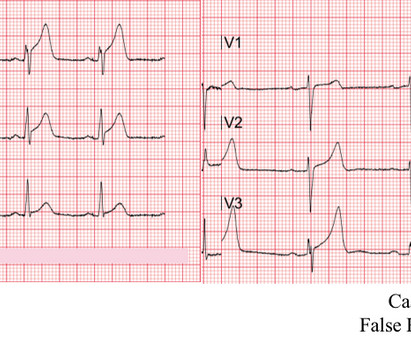
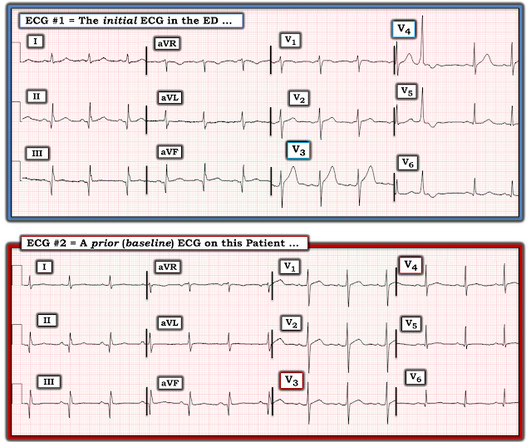
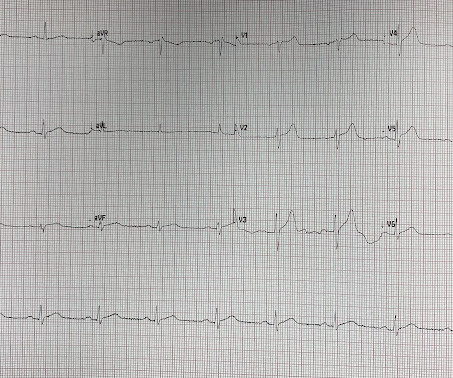
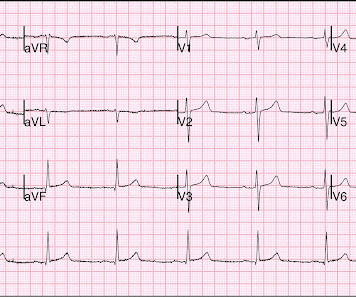
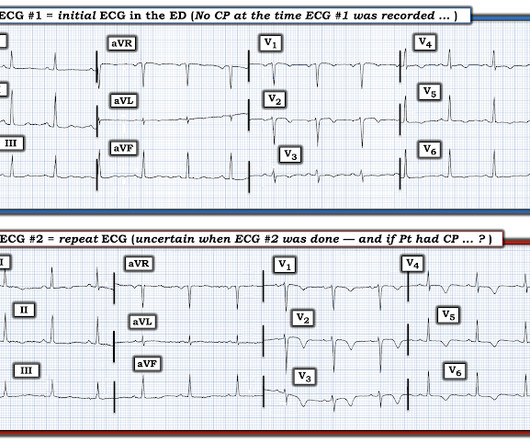
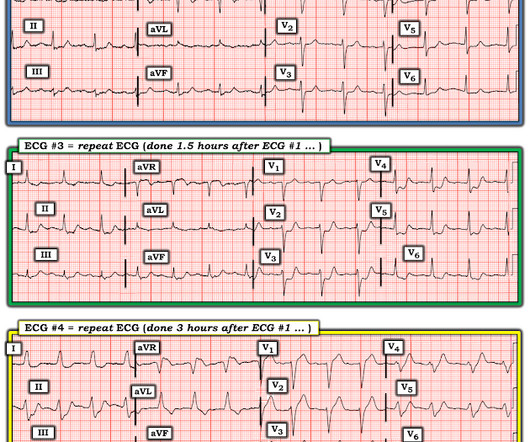
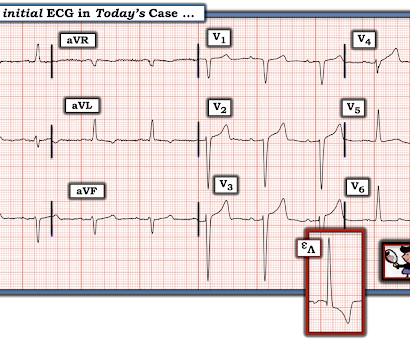
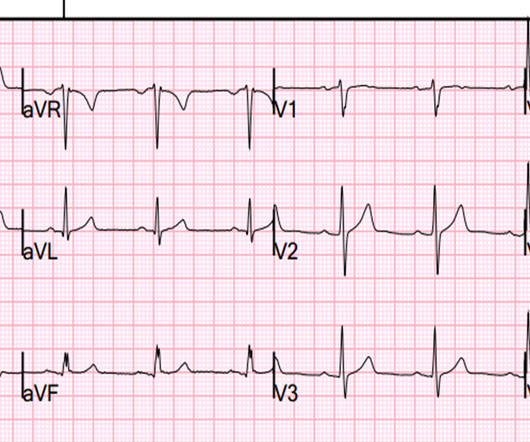
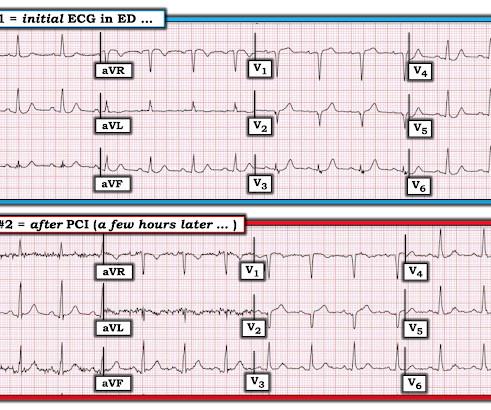
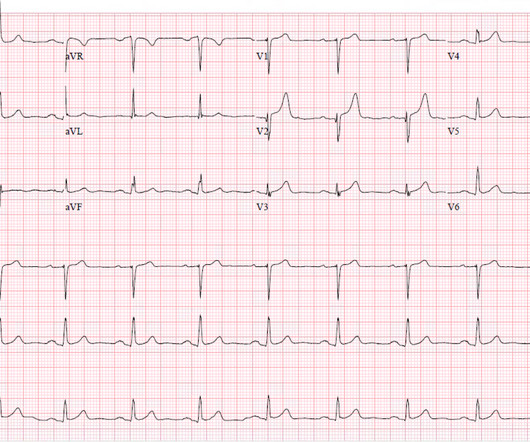
A 41-year-old South Asian male with history of hypertension, alcohol use disorder and hyperlipidemia, who has a strong family history of CAD presented with central substernal burning, pressure, and pain with associated diaphoresis. Coronary angiography before and after intervention is shown below. New PMcardio for Individuals App 3.0
















Let's personalize your content