This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
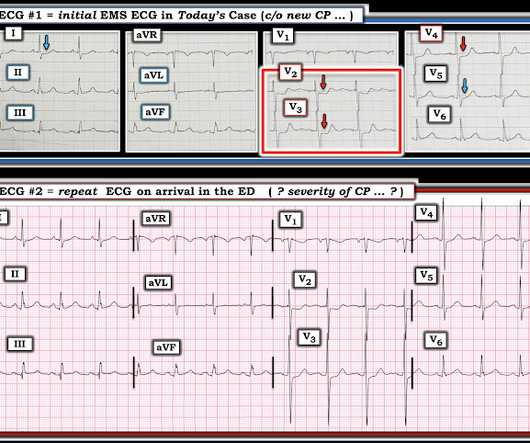
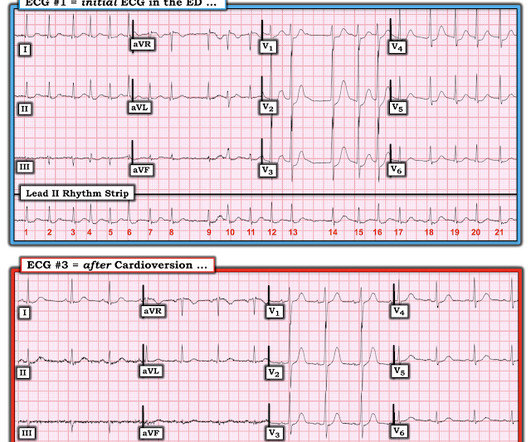
A 60-something with h/o Coronary Bypass called 911 for acute chest pain. On arrival, an ED ECG was recorded: Still diagnostic When a patient has severe chronic coronary disease, findings which appear to be acute can sometimes be chronic, so in this patient with h/o CABG (coronary bypass), it is wise to find a previous ECG if possible.
Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Finally, do a coronary angiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. Coronary Angiography No angiographic significant obstructive disease.
You load him in the back of your ambulance and acquire a 12-lead electrocardiogram (ECG) and it is as follows: You are 5 minutes from a local community hospital and 45 minutes from the tertiary care center with percutaneous coronary intervention (PCI) capabilities. Which hospital do you choose? This speaks to the true essence of the question.
Given the right coronary anatomy seen during angiography, it is particularly interesting that subtle T wave changes were seen on the previous EKGs in the high lateral leads that would otherwise only be expected with a more proximal RCA lesion.
This typically occurs in the setting of a rapidly reperfused coronary artery following a myocardial infarction. The pattern is mostly described with LAD OMI, but has been reported in other coronary distributions as well. The authors recognized this pattern in ~2% of patients with acute anterior MI ( ie , in 30/1532 patients studied ).
Does that normal troponin and ECG obviate the need for cardiology consultation for my patient with a concerning story for acute coronary syndrome? Should I wait for imaging results or labs for this trauma patient before deciding on starting blood or placing a chest tube?
The Journal of Emergency Medicine Neurologic etiologies of cardiac arrest are associated with early withdrawal of life-sustaining therapy Resuscitation Point of Care Echocardiography and Regional Wall-Motion Abnormalities in Acute Coronary Syndromes The Journal of Emergency Medicine Proximal venous ultrasound with risk stratification safely excludes (..)
Rapid re-perfusion of the coronary arteries is essential to save at risk myocardium from infarction in patients with acute coronary artery occlusion. However, patients with occlusions that do not have STE may not activate the system and at least a quarter of the non-STEMI cases have an associated coronary artery occlusion.
Use with caution in neonates with coronary artery disease or chronic nephropathy due to the risk of ischemia and reduced renal blood flow. It is particularly useful in septic shock and should be considered when vasoplegia (low systemic vascular resistance) does not respond adequately to catecholamines.
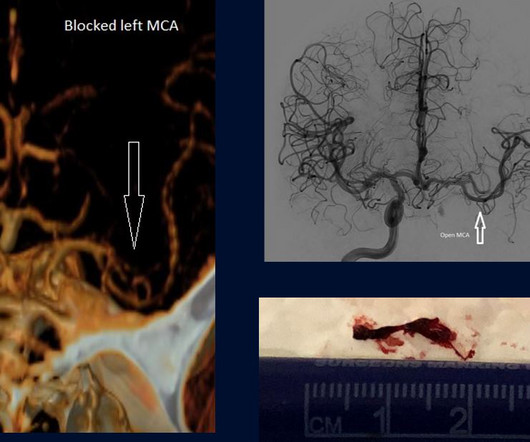
Instead of floating a wire into the heart to remove a clock in a blocked coronary artery to restore blood flow, we were floating wires into people’s brains to remove the clot obstructing blood flow –a life-saving procedure. One of the best things about thrombectomies is they have extended the stroke window out to 24 hours.
She then underwent a CT coronary angiogram : Coronary arteries: all normal, with calcium score of zero However, also seen: Bilateral pulmonary embolus seen in the bifurcation of the left pulmonary artery extending down into the descending branches and in the lingular branch. Right ventricular enlargement with probably reduced function.
A quadruple coronary bypass. Coronary artery disease that had developed over decades. And left untreated, it chips away more than just your mind. It takes your body, too. The Hidden Cost In December 2024—long after I’d retired from the field—I underwent open-heart surgery. Was PTSD the sole cause? Of course not. But did it contribute?
. ► 2015 (188) ► December (16) ► November (16) ► October (15) ► September (15) ► August (20) ► July (13) ► June (15) ► May (11) ► April (19) ► March (21) ► February (9) ► January (18) ► 2014 (151) ► December (15) ► November (15) ► October (11) ► (..)
On arrival, she still had chest pressure and this ECG was recorded: Atrial fibrillation with rapid ventricular response Diffuse ST depression, as with prehospital ECG Is the ischemia a result of atrial fib with RVR, or is atrial fib with RVR just exacerbating ischemia whose source is acute coronary syndrome? She did well overnight.
A middle-aged woman with known severe coronary disease had onset of substernal chest pain while at dialysis. Is this Acute Coronary Syndrome? 2) Very high risk percutaneous coronary intervention 3) Fibinolytic therapy! 911 was called. A prehospital ECG was similar to the first ED ECG, which is shown below.
He was sure the doctors did not tell him that his brother succumbed to occlusion in the coronary arteries. His elder brother died 5 years ago, at the age of 38 years of similar “Hampir Stroke” symptoms. Here is his ED ECG: Day 1, "Hampir Stroke," temp 39 degrees : What do you see? There is ST Elevation in V1-V3, but clearly not due to STEMI.
A pilot randomized controlled study Journal of Critical Care Effect of Ketamine Analgosedation on Neurological Outcome in patients with Severe Traumatic Brain Injury: A Randomized Controlled Pilot Study Neurocritical Care Effects of a general practitioner-led brief narrative exposure intervention on symptoms of post-traumatic stress disorder after (..)
The proposed rationale for this "ventriculophasic" P-P interval variation — is that the P-P interval that contains a QRS complex "sandwiched" within it, tends to be slightly shorter than the P-P interval located away from the QRS — because coronary perfusion will be a little better immediately following ventricular contraction.
See this case in which the ECG which was recorded after stabilization is diagnostic: ST depression, pulmonary edema, and severe hypertension: is this demand ischemia or acute coronary syndrome? In this case, it is reasonable to assume that there is no ACS.
His story was concerning for acute coronary syndrome, so he was admitted to the hospital. Of those 10 that were cath’ed, 9 had significant coronary artery disease and all 9 had significant (>90%) stenosis of the LAD. ECG A was obtained upon arrival to the ER from a 45-year-old male with exertional chest pain. Am Heart J.
The interventionalist stated that a transplanted heart does not have coronary disease. We were aware that ST Elevation can be a result of the low flow state in cardiac arrest, and resolve with time, but we activated the cath lab. A chart review however, revealed the the patient had had an acute distal LAD occlusion one month prior.
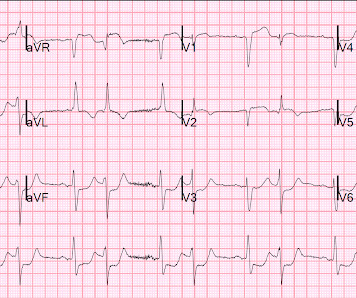
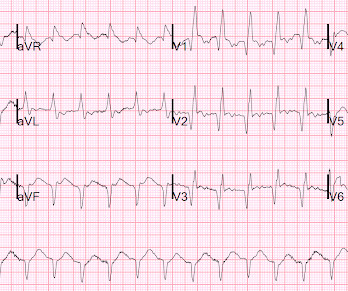
The T wave changes that have occurred are widespread, and not in a typical coronary distribution. Each time the patient underwent cardiac catheterization — and each time, she had patent coronary arteries! Discussion : ECG #2 shows sinus rhythm with quite dramatic change in T wave morphology when compared to ECG #1.
Angiogram: Severe two-vessel coronary artery disease of a left dominant system including 70 to 80% stenosis involving the distal left main/bifurcation. Case continued Troponins over 26 hours, from right to left : Echocardiogram: Mild concentric left ventricular wall thickening, normal cavity size, and normal systolic function.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chest pain. The most common way is by delivering a lead into the coronary sinus ostium in the RA, which wraps around the posterolateral portion of the LV. ECG 1 What do you think?
So we decided this was not acute coronary syndrome. So we electrically cardioverted to sinus rhythm, and recorded another ECG: Now there is only trace residual ST depression. This is good evidence that it was all rate related. The patient was admitted to the hospital. He ruled out for MI. Normal left ventricular cavity size.
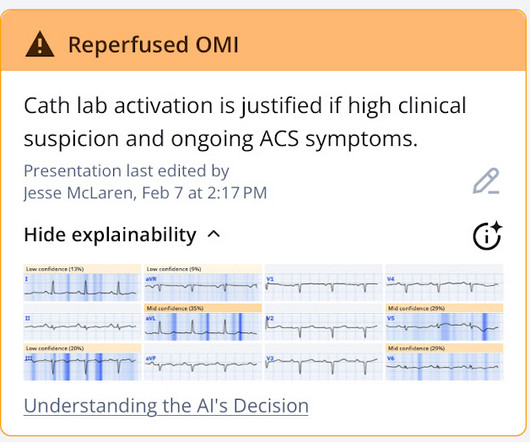
Coronary angiography before and after intervention is shown below. New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. There was high clinical suspicion and ongoing symptoms, so the cath lab was activated.
He discusses how using multiple OMI findings such as acute Q wave, subtle STE, reciprocal STD, hyperacute T waves, and reciprocal TWI to contribute to your overall impression, can double the sensitivity of STEMI criteria for acute coronary occlusion.
Nevertheless, because of the story and because of the recurrent symptoms on medication in the ED as well as the concerning ECG, patient was taken emergently to the Cath Lab, underwent above procedure which showed: 1) Culprit is 100% occlusion of the mid right coronary artery with grade II left to right collaterals.
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI).
A 60-something female with no history of coronary disease or myocardial infarction complained to bystanders that she was dizzy, then collapsed from standing. 911 was called and first responders arrived to find the patient conscious but groggy and disoriented, after which she gradually became more alert and oriented.
As the cath lab report noted, The culprit vessel unfortunately was not clear due to the fact that he has diffuse coronary artery disease. Queen of Hearts of Heart identifies this as acute coronary occlusion: The chest pain resolved after nitro and the ECG was not repeated. So which was the culprit?
Despite the emergence of more advanced support modalities, the IABP continues to serve a critical role in optimizing coronary perfusion and reducing left ventricular (LV) workload.In The intra-aortic balloon pump (IABP) remains a commonly utilized mechanical circulatory support device in the management of cardiogenic shock.
This was presumed to be an isolated acute RV infarction and due to the patient stability and the difficulty of the coronary anatomy, no intervention was undertaken. Coronary Angiograms LMCA : 60% calcified mid to distal LM stenosis. A formal echo showed some RV dysfunction and normal LV anterior wall.
Autolysis and reperfusion the right coronary artery prior to ED presentation was likely responsible for the subtle biphasic terminal T wave inversion seen on his presenting ECG. 12 hours after presentation the right coronary artery likely RE-occluded, manifesting in the clear ST segment elevation myocardial infarction seen at 2:00 AM.
. ► October (11) ► September (15) ► August (11) ► July (13) ► June (8) ► May (12) ► April (14) ► March (13) ► February (9) ► January (15) ► 2013 (120) ► December (14) ► November (9) ► October (10) ► September (9) ► August (13) ► July (9) ► June (..)
. ► April (16) ► March (19) ► February (8) ► January (18) ► 2018 (188) ► December (11) ► November (18) ► October (16) ► September (16) ► August (13) ► July (19) ► June (13) ► May (12) ► April (23) ► March (16) ► February (16) ► January (15) ► (..)
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management.
. ► January (23) ► 2015 (188) ► December (16) ► November (16) ► October (15) ► September (15) ► August (20) ► July (13) ► June (15) ► May (11) ► April (19) ► March (21) ► February (9) ► January (18) ► 2014 (151) ► December (15) ► November (15) ► (..)
. ► March (19) ► February (8) ► January (18) ► 2018 (188) ► December (11) ► November (18) ► October (16) ► September (16) ► August (13) ► July (19) ► June (13) ► May (12) ► April (23) ► March (16) ► February (16) ► January (15) ► 2017 (153) ► (..)
10 g/dL in patients with acute coronary syndrome (ACS). While permissive hypotension may be a helpful strategy in some clinical scenarios, blood product resuscitation should generally continue for a MAP of 65 and clinical improvement such as improvement in mental status and distal extremity perfusion.
An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. 65 y old male, hypt, IHD, smoker, central chest pain, was in pulm oedema Killip III Great recent article relevant to this: Kosuge M, Ebina T, Hibi K, et al. Am J Cardiol;107(4):495-500.
. ► June (13) ► May (12) ► April (9) ► March (9) ► February (12) ► January (22) ► 2019 (181) ► December (11) ► November (16) ► October (12) ► September (11) ► August (18) ► July (19) ► June (16) ► May (17) ► April (16) ► March (19) ► February (..)
. ► 2016 (142) ► December (8) ► November (16) ► October (10) ► September (9) ► August (12) ► July (6) ► June (11) ► May (11) ► April (8) ► March (16) ► February (12) ► January (23) ► 2015 (188) ► December (16) ► November (16) ► October (15) ► (..)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content