This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This was written by one of our fine residents, who will soon be an EMS fellow: Michael Perlmutter Case A mid-50s male came to the ED with a burning sensation that was acutely worse while at home. He came to the ED at the urging of his wife.
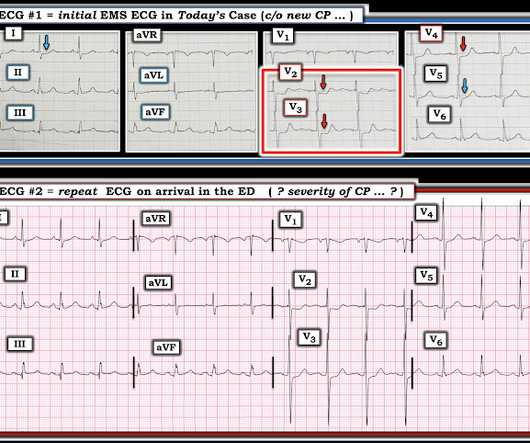
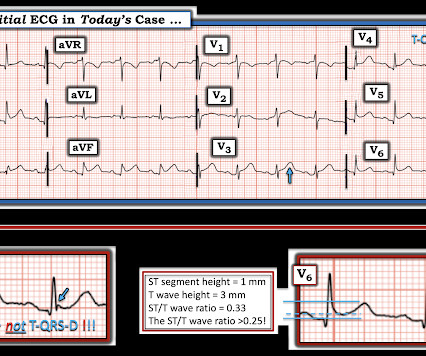
A 60-something with h/o Coronary Bypass called 911 for acute chest pain. On arrival, an ED ECG was recorded: Still diagnostic When a patient has severe chronic coronary disease, findings which appear to be acute can sometimes be chronic, so in this patient with h/o CABG (coronary bypass), it is wise to find a previous ECG if possible.
Rapid re-perfusion of the coronary arteries is essential to save at risk myocardium from infarction in patients with acute coronary artery occlusion. However, patients with occlusions that do not have STE may not activate the system and at least a quarter of the non-STEMI cases have an associated coronary artery occlusion.
She then underwent a CT coronary angiogram : Coronary arteries: all normal, with calcium score of zero However, also seen: Bilateral pulmonary embolus seen in the bifurcation of the left pulmonary artery extending down into the descending branches and in the lingular branch. Right ventricular enlargement with probably reduced function.
A middle-aged woman with known severe coronary disease had onset of substernal chest pain while at dialysis. A prehospital ECG was similar to the first ED ECG, which is shown below. Here is her initial ED 12-lead ECG: There is atrial fibrillation with a rate of approximately 114. Is this Acute Coronary Syndrome?
He was sure the doctors did not tell him that his brother succumbed to occlusion in the coronary arteries. Here is his ED ECG: Day 1, "Hampir Stroke," temp 39 degrees : What do you see? His elder brother died 5 years ago, at the age of 38 years of similar “Hampir Stroke” symptoms. This is Classic Type I Brugada Morphology.
Angiogram: Severe two-vessel coronary artery disease of a left dominant system including 70 to 80% stenosis involving the distal left main/bifurcation. How many patients do not present to the ED until the next day? The estimated left ventricular ejection fraction is 64%. There is no left ventricular wall motion abnormality identified.
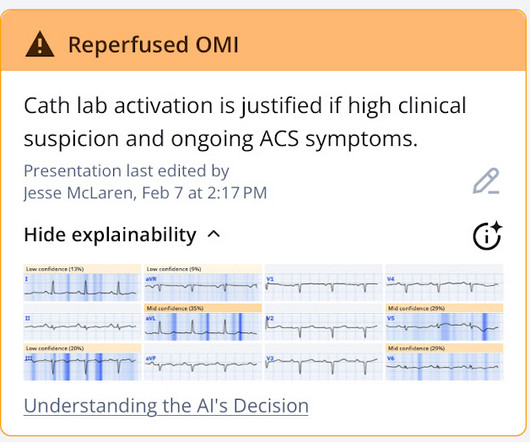
Coronary angiography before and after intervention is shown below. New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. There was high clinical suspicion and ongoing symptoms, so the cath lab was activated. The rhythm is sinus.
2 days prior to presentation to the ED, started having chest tightness which he thought was secondary to the persistent coughing, muscular ache type pain. Pt denies family history of AMI. His pain is 9/10. 50-something gentleman with three week history of common cold symptoms with persistent coughing.
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis What do you think?
As the cath lab report noted, The culprit vessel unfortunately was not clear due to the fact that he has diffuse coronary artery disease. Queen of Hearts of Heart identifies this as acute coronary occlusion: The chest pain resolved after nitro and the ECG was not repeated. So which was the culprit?
A 60-something female with no history of coronary disease or myocardial infarction complained to bystanders that she was dizzy, then collapsed from standing. First ED ECG: There is ST Elevation in V2 which appears ischemic. Patient had no memory of event. Exam was normal. There is terminal T-wave inversion suggesting reperfusion.
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management.
Here is his ED ECG (compare with the 2 month previous ECG below it): --Is there a new Q-wave (tiny r-wave) in III? This was presumed to be an isolated acute RV infarction and due to the patient stability and the difficulty of the coronary anatomy, no intervention was undertaken. Chest pain was not relieved by sublingual NTG.
This was written by Mark Hellerman, Cardiology Fellow at Stony Brook: The Case: A 60 year old man with no reported medical history presents to the ED for evaluation of chest pain. The Case In this case, it is likely that the patient auto-lysed a culprit lesion prior to presentation to the ED.
Case: A 32-year-old female presents to the ED with chief complaint of abdominal pain. 10 g/dL in patients with acute coronary syndrome (ACS). Well keep it short, while you keep that EM brain sharp. Her pain started 8 hours ago and became severe within the last 30 minutes. C, and 20 respirations/min.
The physician was worried about possible acute coronary occlusion, and activated the cath lab. The angiogram showed no significant coronary disease: First troponin I was 10 ng/L. Louis University, presented at Heart Rhythm Society: 1 month of chest pain in the ED. Download now for iOS or Android. Second troponin was 23 ng/L.
This is really good Prehospital, ED, and Cardiolog. Fever, tachycardia, hypotension, hypoxia and "SVT" A woman in her 40s with palpitations and chest pre. Flecainide toxicity 4/21/21 2597782 This case was flagged as a false positive cath lab. A man in his 60s with diaphoresis, vomiting, and i.
Question and Methods: The Authors assessed whether a 0/1-hour high-sensitivity troponin protocol increased safe ED discharges compared to standard 0/3-hour care, using a stepped-wedge, randomized trial across 9 US EDs.
👉 Click here to access the PERC RULE on MDCalc 👉 Click here to access the Wells’ Criteria on MDCalc 🤕 Case A 35 year old woman with no past medical history presents to the ED with pleuritic chest pain and shortness of breath. She is tachypenic but has a normal heart rate and oxygen saturation.
Between 6-9 million patients present to the ED for chest pain annually. Objectively risk-stratifying these patients may help guide management and optimize resource utilization, resulting in shorter hospital and ED stays for low risk patients, and earlier interventions for moderate- and high-risk patients.
Acute coronary occlusion seen in paced *and* non-p. Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Danika Atrial fib RVR case in text message and inb. A 40-something male complains of worrisome chest p.
Ed Burns (from Life in the Fast Lane) sent me this. A 50-something with h/o coronary bypass has chest. See what happens when one fails to diagnose STEMI. Serial ECG recordings are essential: paramedic mak. Are These Wellens' Waves?? Repost this one great atrial tach case Early repol with increasing STE, formula values ve.
An 86-year-old man with a history of hypertension, hyperlipidemia, cardiomyopathy, and our-vessel coronary artery bypass five years prior presented to the emergency department (ED) with one hour of sudden-onset retrosternal, pressure-like chest pain radiating to the left arm. The ECG obtained in the ED is shown above.
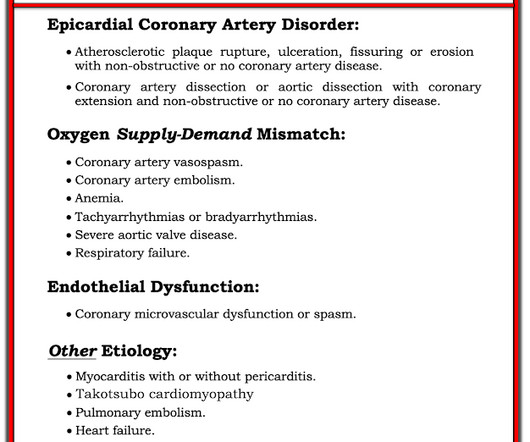
Denies family hx of coronary artery disease and premature cardiac death. Other DDX include, but less likely, coronary spasm, plaque rupture, and coronary microvascular dysfunction. On the arrival to ED, patient with ST elevations and elevated Troponin. She is on lisinopril and metformin.
ED echo: The left ventricular ejection fraction appears: Severely reduced No pericardial effusion identified. Emergency physicians never want to miss an acute coronary occlusion, and cardiologists hate angiograms that, in retrospect, were unnecessary. There was clearly a myocardial infarction and severe coronary disease.
Emergency (ED placement) Transvenous Pacer appears. Back to basics: what is this rhythm? What are your. 30 yo woman with trapezius pain. HEART Pathway =. Good case for showing a flutter and LBBB, Good cas. What is this rhythm? Back to basics. Is there Terminal QRS Distortion? What is so unusual about this inferior OMI (which.
A 47 year old with 2 hours of somewhat worrisome sounding chest pain presented to the ED. He was a smoker but had no other coronary risk factors. or your suspicion for coronary occlusion is other wise high, it is wise to evaluate intensively. Is this a proximal occlusion of a wraparound LAD, or is it just a normal variant?
Intubated External pacing To cath lab Coronaries ok Pacemaker Posted by Steve Smith at 8:16 AM Email This BlogThis! Share to X Share to Facebook Share to Pinterest Labels: draft No comments: Post a Comment DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them.
Dysnpea and Elevated troponin Takotsubo that looks like LVA Huge Precordial ST Elevation in an ED Patient Tachycardia, hyperthyroid, and ST elevation. Is this just right bundle branch block? Besides the Nonspecific T-wave Inversion in aVL, W.
Chest pain resolved, and a "Normal" ED ECG 2 cases of false pos STE aVL What will you do for this patient transferred to y. 30-something male with confusion, weakness, headac. A Patient with Respiratory Failure and a Computer. Cardiac arrest with STEMI pattern: no acute corona. How accurate are the Monitor leads for ST Elevation?
A 12-lead electrocardiogram (ECG) demonstrates ST elevations in leads II, III, and aVF with ST depressions in leads I and aVL and the team begins transport to the nearest percutaneous coronary intervention (PCI) capable hospital. We looked at 101 STEMI patients from two rural EDs. Reference: Stopyra et al.
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
Sepsis) De Winters T waves are the earliest sign of an anterior wall MI but will only be present in ~ 2% of LAD infarcts Patients with Wellens Syndrome on ECG should have a cardiac cath within 24 hours, not necessarily within the first 60 minutes of ED arrival.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain.
In this month's EM Quick Hits podcast: Megan Landes on the importance of diagnosing HIV in the ED, Jesse McLaren on the failed paradigm of STEMI criteria and ECG tips to identify acute coronary occlusion, Anand Swaminathan on evidence for non-invasive airway management in the poisoned patient, Brit Long and Hans Rosenberg on the identification, workup (..)
The Case A 41-year-old male presents to the ED with constant palpitations for one day. Risk factors that increase the likelihood of VT include history of previous myocardial infarction, known coronary artery disease, and structural heart disease. When in doubt, treat as ventricular tachycardia.
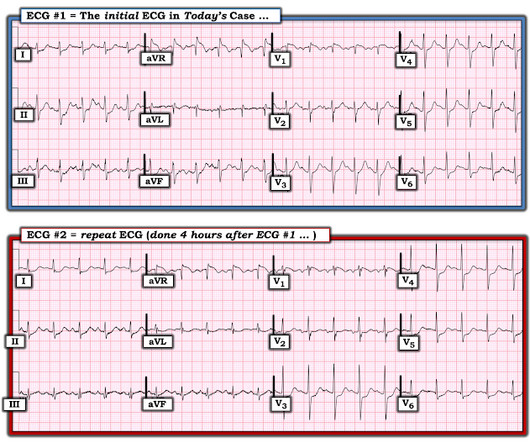
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. It’s judicious, then, to arrange for coronary angiogram.
The Case A 62-year-old male with a history of Hypertension, Hyperlipidemia, Coronary Artery Disease with stents, Pulmonary Embolism on Eliquis, presents with sudden onset, severe, mid-sternal chest pain that started 15 minutes prior to arrival. Discussion Case Discussion: The patient’s history was concerning for an acute coronary syndrome.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content