This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
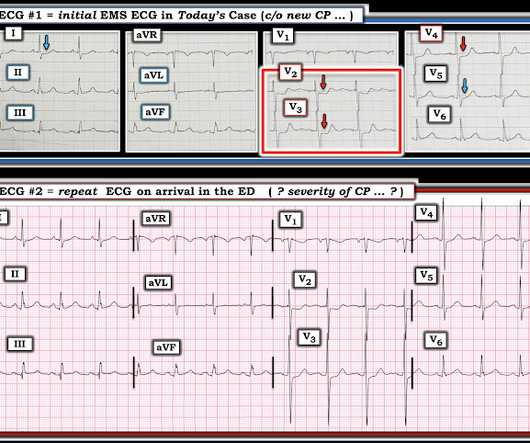
You load him in the back of your ambulance and acquire a 12-lead electrocardiogram (ECG) and it is as follows: You are 5 minutes from a local community hospital and 45 minutes from the tertiary care center with percutaneous coronary intervention (PCI) capabilities. However, the notion of “STEMI equivalents” has gained traction.
A 60-something with h/o Coronary Bypass called 911 for acute chest pain. The Zoll algorithm impressively stated: STEMI A paramedic student had the PMCardio AI Queen of Hearts on his phone and this is what it reported: New PMcardio for Individuals App 3.0 Here is the first prehospital ECG: What do you think?
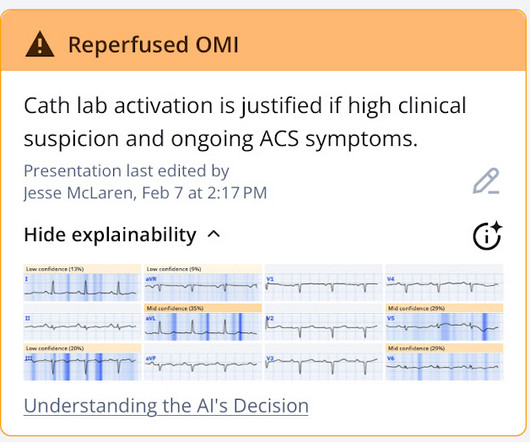
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. This typically occurs in the setting of a rapidly reperfused coronary artery following a myocardial infarction. There is a de Winter T- wave pattern also in lead I.
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. Later in the night, the patient became bradycardic and developed a Mobitz II pattern , but he remained asymptomatic and hemodynamically stable.
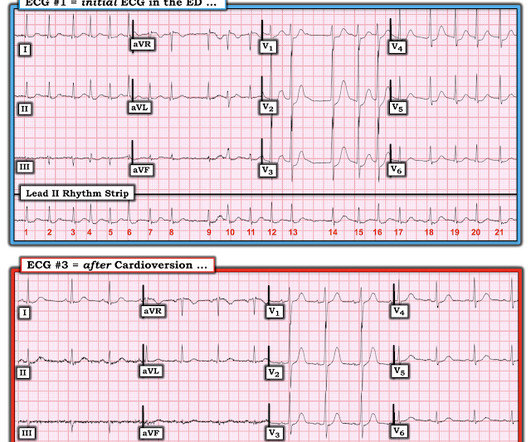
On arrival, she still had chest pressure and this ECG was recorded: Atrial fibrillation with rapid ventricular response Diffuse ST depression, as with prehospital ECG Is the ischemia a result of atrial fib with RVR, or is atrial fib with RVR just exacerbating ischemia whose source is acute coronary syndrome? She did well overnight.
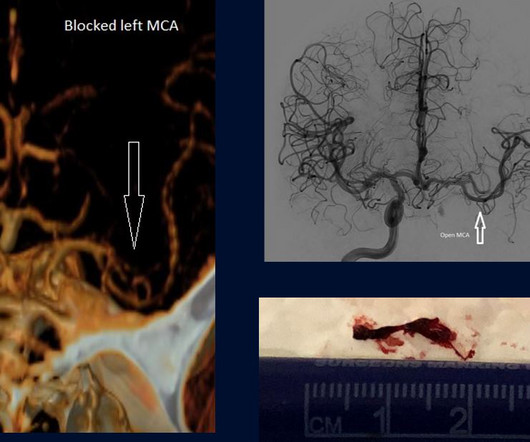
Instead of floating a wire into the heart to remove a clock in a blocked coronary artery to restore blood flow, we were floating wires into people’s brains to remove the clot obstructing blood flow –a life-saving procedure. One of the best things about thrombectomies is they have extended the stroke window out to 24 hours. Again, true.
Rapid re-perfusion of the coronary arteries is essential to save at risk myocardium from infarction in patients with acute coronary artery occlusion. ST-segment Elevation Myocardial Infarction (STEMI) criteria have been the traditional method of cath lab activation.
A middle-aged woman with known severe coronary disease had onset of substernal chest pain while at dialysis. Is this Acute Coronary Syndrome? 2) Very high risk percutaneous coronary intervention 3) Fibinolytic therapy! 911 was called. A prehospital ECG was similar to the first ED ECG, which is shown below.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Inferior STEMI with AV Block, Cardiogenic Shock an. The QRS proves it. Posted by Steve Smith at 6:29 AM Email This BlogThis! Patient dies. Atrial Fib with RVR.
He was sure the doctors did not tell him that his brother succumbed to occlusion in the coronary arteries. There is ST Elevation in V1-V3, but clearly not due to STEMI. His elder brother died 5 years ago, at the age of 38 years of similar “Hampir Stroke” symptoms. This is Classic Type I Brugada Morphology.
He discusses how using multiple OMI findings such as acute Q wave, subtle STE, reciprocal STD, hyperacute T waves, and reciprocal TWI to contribute to your overall impression, can double the sensitivity of STEMI criteria for acute coronary occlusion.
ECG B shows you some abnormal looking T waves that don’t meet STEMI criteria. Finally, ECG C shows an anterior STEMI! ” “Correct. His story was concerning for acute coronary syndrome, so he was admitted to the hospital. V2 and V3 look biphasic. Now let me tell you about this patient. ECG B was obtained 23 hours after admission.
A prehospital ECG showed ST Depression in V1-V3 and the medics were concerned for posterior STEMI. So we decided this was not acute coronary syndrome. Charts showed a history of some mitral regurgitation and an enlarge left atrium, as well as hypertension treated with a thiazide diuretic. Pulse was 128 and irregular, BP was 141/75.
Now as an intern, he is exceptional at EKG interpretation because he was able to learn of the OMI paradigm and importance of pattern recognition before getting poisoned by years of learning STEMI. This is really a transient OMI (or transient STEMI if one uses that terminology and it has diagnostic ST Elevation).
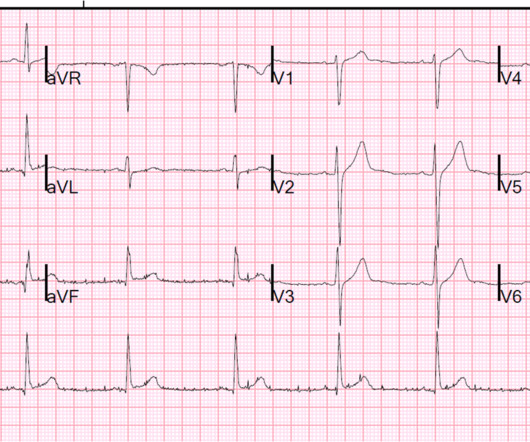
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
As the cath lab report noted, The culprit vessel unfortunately was not clear due to the fact that he has diffuse coronary artery disease. Queen of Hearts of Heart identifies this as acute coronary occlusion: The chest pain resolved after nitro and the ECG was not repeated. Discharge diagnosis was Non-STEMI.
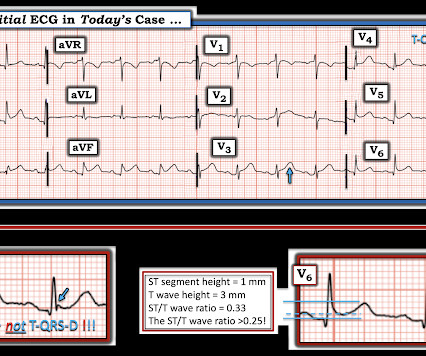
This is almost certainly an acute inferior MI, though does not meet mm "criteria" for STEMI --The beginnings of T-wave inversion suggest an open artery. Because this "anterior" MI is due to STEMI of the right ventricle (RV) , not of the LV. ng/mL due to the brief RV STEMI. It may be due to RV STEMI, which is also anterior.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. hours of chest pain Chest Pain and Right Bundle Branch Block Is this acute STEMI? Is this inferor STEMI? Cardiologist declines taking patient to the cath lab.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. A Middle-Aged male with Chest Pain and an Unusual ECG Doctor, should we activate the hospital's "STEMI a. Cardiologist declines taking patient to the cath lab.
Importantly, one trial of 925 consecutive STEMI-positive occlusion myocardial infarctions found that 26% had presentation troponin values < 99th percentile when then presented less than 2 hours from symptom onset and 14% had values < 99th percentile when they presented with symptoms for greater than 2 hours.
This ECG was recorded 30 minutes later with ongoing pain: Queen of Hearts says no signs of STEMI or Equivalent for both: New PMcardio for Individuals App 3.0 The physician was worried about possible acute coronary occlusion, and activated the cath lab. The angiogram showed no significant coronary disease: First troponin I was 10 ng/L.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Severe RVH with large RV on echo, not a PE "I have food poisoning" Article on STEMI vs. BER Why is there ST depression in aVL in this case of. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. The delay between OMI and STEMI claims yet another. Brugada with superimposed anterior STEMI Chest pain. Cardiologist declines taking patient to the cath lab.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Updated 1 hour lecture: The False STEMI-NonSTEMI D. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. A very fast narrow complex tachycardia in an Infant Do patients with LBBB and STEMI, when reperfused, awesome repost: repost: [link] Rick Abbott case DSECGB: ST resolution.
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Sunday, August 25, 2013 Anterior ST Elevation - Is it STEMI?
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies. .
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies.
Final read: This ECG is concerning for an inferolateral STEMI! Shannon, this looks like a STEMI, activate the cath lab, please!” Mr. Jackson is a 62 year old male coming in with the ECG we sent you pretty concerning for a STEMI, but here’s the problem” … static …. Can you have so much strain that you get a STEMI?
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies. .
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. anterior STEMI, VT, head bleed from stab conf, Cou. ng/ml) Posted by Steve Smith at 12:32 PM Email This BlogThis! Cardiologist declines taking patient to the cath lab.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Left Bundle Branch Block with Subacute STEMI Is this Type 2 Brugada syndrome/ECG pattern? Five Primary Patterns of Ischemic ST depression, without ST elevation.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies. .
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies. .
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. A 20-something male with acute chest pain Inferior STEMI with and without pacing, post ROSC A patient with chest pain that is resolving. . Patient dies.
EKG did not meet clear diagnostic criteria from STEMI. I don't see any evidence of STEMI here. The cath lab was activated and the coronaries were normal. Procedure: Coronary angiography. JL-4 catheter for the left coronary artery Attempts were made to engage the RCA with an AL-1, CAS-1 and CAS-2 without success.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Max Palatnik case Is this Septal STEMI/OMI? Acute coronary occlusion seen in paced *and* non-p. Patient with STEMI (-) OMI is now pain free. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. A 30-something with It is not a STEMI; it is an opportunity to save my. Is this acute coronary occlusion? Cardiologist declines taking patient to the cath lab.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. See what happens when one fails to diagnose STEMI. A 50-something with h/o coronary bypass has chest. . Cardiologist declines taking patient to the cath lab.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies. .
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies. .
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content