This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Guest Skeptic: Missy Carter is a PA currently practicing in criticalcare after having attended the University of Washington's MEDEX program. The Paramedic 3 Trial: A randomized clinical trial of drug route in out-of-hospital cardiac arrest. October 31, 2024 NEJM Access to the SGEM Podcast episode at this LINK. Reference: Couper et al.
We’re excited to announce the launch of our advanced CriticalCare functionality within ESO Electronic Health Record (EHR) , designed to meet the unique demands of high-acuity healthcare environments. Advanced Reporting and Analytics Understanding the data behind your care drives ongoing improvement.
Criticalcare admission is typical for hemodynamic monitoring and support. Five Key Take-Home Points High Suspicion Saves Lives: Recognize severe pain out of proportion as a critical red flag. We discuss the recognition and treatment of necrotizing fasciitis. Bacteroides, Clostridium, Peptostreptococcus).
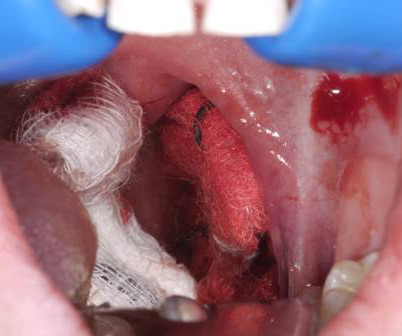
The key is a stepwise, three-pronged approachresuscitation, early ENT consultation with transport arrangements, and temporizing measures applied to control bleedingto keep the patient safe until shes transferred to definitive care. Her vital signs are normal, except for a heart rate of 115 bpm. CREDIT: Dr. P.
The guide concludes with the critical final step of determining the capture threshold to ensure effective and safe pacing. This video is perfect for emergency medicine and criticalcare providers looking to master or refresh their skills on this life-saving procedure. Read More
Journal of Hepatology Association of central capillary refill time with mortality in adult trauma patients: a secondary analysis of the crash-2 randomised controlled trial data Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine Dorsal Digital Nerve Block Versus Ultrasound-Guided Selective Peripheral Nerve Block for Finger Analgesia: (..)
Welcome to CriticalCare Time, a new criticalcare-focused column from ACEP Now. My goal in this column is to share tips, tricks, and emerging concepts from the intensive care unit (ICU) that you can use on your next shift in the emergency department (ED). This column is for you! Unanticipated hypotension.
Emergency medical services(EMS) has historically been a punitive system, resulting in people being unforthcoming about issues or concealing minor infractions in hopes of evading discipline. In a profession as noble as ours, is this what we want? When investigating an incident, identifying the root cause is essential.
Editorial: The Way to a Patient’s Heart – Vascular Access in Cardiac Arrest Question and Methods: This RCT compared IO vs. IV vascular access in adults with OHCA, using ROSC as a primary outcome.
Both studies demonstrated no difference in their primary outcome of mortality before discharge home by day 90 when employing a ‘liberal’ or ‘restrictive’ approach to fluid resuscitation for patients in septic shock. LVOT VTI is particularly helpful in managing septic patients because it offers a reliable way to evaluate fluid responsiveness.
Current care modalities for patients are primarily centered on medical stability during transport and do not adequately address aspects such as patient comfort or alignment with goals when a patient is on hospice or at risk for delirum.
Despite a high mortality rate (60% at 180 days) potentially underestimating long-term risks, the study's robust design supports IO access as a generally safe and effective procedure in criticalcare situations. The post What’s the long term complication rate of IO access?
The study compared the effects of different albumins on improving heart function and reducing fluid requirements during critical resuscitations. The findings were promising. ” Whether responding in urban environments or remote rural areas, a lightweight, easy-to-store solution like 25% HSA could prove invaluable.
Rethinking the Recruitment Model—People Hire People Memphis Fire and Rescue shifted recruitment responsibility from traditional human resources personnel to firefighters and firefighter-paramedics deeply embedded in the culture.
This distinction is critical: EMS providers should rely on their specific guidelines, which consider the operational environment and exposures inherent to prehospital care, rather than hospital rules designed for prolonged patient contact. Surgical masks, combined with proper vehicle ventilation protocols, suffice for most encounters.
Frequently, point-of-care ultrasound (POCUS) is utilized to evaluate ejection fraction and for B-lines, but evaluating for these alone does not answer the full question. That is, it may provide a measure for when fluid resuscitation should be stopped and earlier pressors utilized.
Barriers to Treatment Remain High Despite the clear need, many first responders hesitate to seek mental health care due to stigma and fear of professional consequences. The study highlighted concerns that seeking help might lead to being labeled “weak,” losing one’s license, or being sidelined at work.
Day 1 • Didactic presentations by Dr. Levitan and Dr. Rezaie on crisis performance, oxygenation, airway anatomy, laryngoscopy, endoscopy, pediatrics, rescue oxygenation techniques and criticalcare. End of day will involve discussion of challenging airway management cases from participants and faculty.
0000000000004651] Bellal Joseph, MD FACS Dr. Bellal Joseph is the Martin Gluck Endowed Professor of Surgery, Professor of Neurosurgery, Chief of General Surgery and Chief Division of Trauma, CriticalCare, Burns & Emergency Surgery, at the University of Arizona. Questions Before Joining (FAQ) Join Now!
About PICSTAR PICSTAR is a trainee-led research network open to all doctors, nurses and allied health trainees within Paediatric Intensive Care. We are the trainee arm of the Paediatric CriticalCare Society – Study Group (PCCS-SG) and work with them on research, audit and service evaluation.
Author : Daniel Johnson, DO, FACEP; Assistant Professor, Department of Emergency Medicine, Life Lion EMS & CriticalCare Transport, Penn State Health Milton S. In 2018, Meyers, Weingart, and Smith published “The OMI Manifesto” which shed light on the concept of a novel categorization of acute myocardial infarction 2.
Adrenaline, an endogenous catecholamine produced by the adrenal medulla, exerts its effects on both alpha- and beta-adrenergic receptors in a dose-dependent manner, triggering the well-known sympathomimetic ‘fight or flight’ response to stress. It should be delivered intravenously, or if intravenous access is unavailable, via the intraosseous route.
Pathophysiology I know we all tend to skip the pathophysiology bit when revising (or maybe it was just me) but bear with me, I promise it will make treating hypotension a little easier. Systemic Vascular Resistance (SVR): Neonatal immature autonomic regulation can lead to failures in vascular tone maintenance, resulting in low SVR.
EHR | FLACC Pain Scale The FLACC Pain Scale was part of our CriticalCare initiative in 2024 and will be available in the Pain section within Vitals in ESO EHR. You can now automatically calculate Shock Index based off of the values you enter for Pulse and Systolic Blood Pressure.
Auto-Generated Narrative is just one of ESO EHRs new innovative features aimed at empowering first responders in better caring for their communities. By drawing directly from structured data already entered in the record, ESOs Auto-Generated Narrative writes a full narrative summary ready for review.
Light has 30 years in the field of EMS, with a background in criticalcare. 5 min read News News Feed Patient Care Headlines Nebraska Whole Blood Massachusetts Opioid Overdose Deaths Down 36% in 2024 Opioid related overdose deaths fell 36% in Massachusetts in 2024, reaching their lowest point since 2013.
In addition to the reduced risk for major bleeding, use of mechanical thrombectomy techniques has been shown to decrease hospital costs by reducing the need for post-procedural criticalcare following intervention. A massive PE, the most severe, causes hemodynamic instability and carries the most morbidity and mortality.
Other prehospital clinicians included Emergency care assistants ( 7% ) and student paramedics ( 8% ) (see Figure 1 ). These cases often involved criticalcare, multiple specialist teams, and more complex diagnoses or prognoses. Neurological diagnoses What do prehospital clinicians think of the feedback survey?
Prehospital clinicians are often the first to assess and treat critically unwell children, making crucial decisions under pressure and initiating vital interventions. Many prehospital clinicians report feeling anxious and lacking confidence when caring for younger patients. e.g., ST3 + (UK equivalent).
The ability to move sensitive medical cargo quickly and reliably improves overall patient care efficiency and reduces operational bottlenecks. Their Guardian system can deliver critical emergency supplies—Narcan, epinephrine, blood products, AEDs—direct to incident scenes faster than ground crews can arrive.
Paramedics are increasingly required to assess patients and determine whether they can be safely managed at home with self-care or primary care or if they need to be transferred to the hospital. The researchers used electronic health records to identify VZV complications seen in secondary care. What is chickenpox?
This contributes to feelings of isolation and insufficient support during critical times. Stacee shared stories collected anonymously from frontline women experiencing miscarriages, fertility struggles and chronic conditions like endometriosis—all while navigating the physical demands of the job.
IF YOU OR A LOVED ONE NEEDS HELP, CALL 988 OR SEEK CARE AT A LOCAL EMERGENCY DEPARTMENT. WE, AS EMS PROFESSIONALS, SHALL PROVIDE COMPASSIONATE, APPROPRIATE CARE TO ALL PATIENTS. TRIGGER WARNING: TOPICS OF SUICIDE MAY BE HARD FOR SOME PEOPLE TO READ ABOUT. THIS ARTICLE IS COVERING THE MEDICAL ASPECTS OF CHEMICAL SUICIDES.
Operating 24/7/365, GundersenAIR responds to high-acuity emergencies when ground transport is impractical or time-sensitive care is required in flight. Both solutions significantly improve patient care by ensuring precise weight-based dosing and streamlined adherence to medical protocols.
Welcome to the first episode of the Broomedocs podcast for 2025. Justin and I are back for more nerdy goodness to make you smarter in the Resus room, or at a pub trivia night more likley… wether it is about salt correction, dissection or infection we can help you out! Listen in and learn! Dimer is useful in the low risk group. Emerg Med J.
found no difference in mortality in criticalcare patients treated with vancomycin and piperacillin- tazobactam compared to vancomycin and cefepime or meropenem. found no difference in mortality in criticalcare patients treated with vancomycin and piperacillin- tazobactam compared to vancomycin and cefepime or meropenem.
He has 33 years of EMS experience, beginning in the early 1990s, having been certified at various times as a an EMT, an EMT-I, a criticalcare technician and a paramedic. This was called CriticalCare Technician. Kroll says there are any additional liability issues with using three levels of provider at his agency.
4 min read Admin/Leadership Podcasts EMS EMT Paramedic The JEMS Report Gwenny Winkler on CriticalCare, Coaching and Embracing Growth Veteran flight nurse and educator Gwenny Winkler shares her EMS journey.
9 min read Commentary Exclusives Patient Care EMS EMT Paramedic Being a Better Advocate for Your Patients with Developmental and Intellectual Disabilities An EMS provider with autism shares insights on effectively responding to patients with autism and developmental or intellectual disabilities.
Burn center consultation; need center with multidisciplinary care (criticalcare, dermatology, burn surgery, ophthalmology, ENT, pulmonology, gastroenterology, nephrology, urology, gynecology, psychiatry, wound care, and nutrition). Chronic phase: disease stops progressing in convalescent stage, then recovery stage.
This approach builds critical thinking skills and helps providers work through complex scenarios independently—crucial in both exams and the field. This is sobering but reassuring advice for any EMS clinicians eager to expand their scope into criticalcare transport.
Skip to content Twitter Google+ Facebook Reddit RSS The Bottom Line A compendium of critical appraisals in Intensive Care Medicine research and related specialties Home About Us Summaries Intensive Care Medicine Emergency Medicine Peri-operative Medicine Blog News EBM Editorial Submit a review Wessex ICS You are here: Home Blog CriticalCare Evidence (..)
Patients were randomised in a 1:1 ratio to receive either nasal high-flow or standard care. 1069 intubations in 969 children were randomly assigned to nasal high flow (535 intubations) or standard care (534 intubations). Children who required multiple intubations could be re-enrolled and re-randomised.
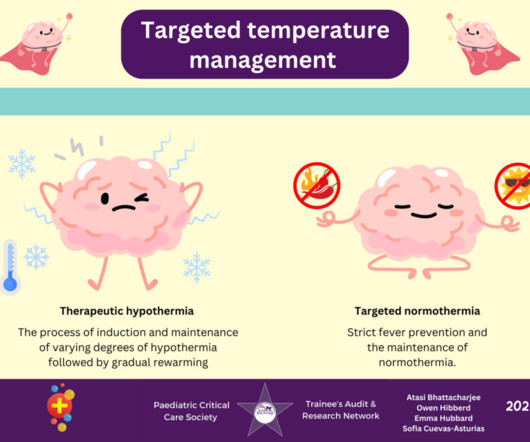
ACNS divides NCSE in the critically ill patient into electrographic status epilepticus and electroclinical status epilepticus. Two forms: 1) convulsive SE (CSE) marked by prominent motor activity, and 2) non-convulsive SE (NCSE) without prominent or clinically obvious motor activity. Recently this definition has been modified to 10 minutes.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content