This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This was written by one of our fine residents, who will soon be an EMS fellow: Michael Perlmutter Case A mid-50s male came to the ED with a burning sensation that was acutely worse while at home. He came to the ED at the urging of his wife.
Here is the prehospital ECG: The computer says STEMI Based on this and the presence of chest pain, the medics did a prehospital activation of the cath lab. A 40-something male complained of 3 days of chest pressure. He called 911. He had some pulmonary edema and hypoxia. What do you think? Interpretation: There is clear atrial flutter.
interesting spontaneous reperfusion case 1413140 prehospital STEMI first ED ECG is here, with 3/10 pain: But this is the same patient just 10 minutes before, with 7/10 pain Isn't it ridiculous to say that the patient has both a STEMI and an NSTEMI? ACS is dynamic. It can't be given one static name.
Diagnosis: Atrial Fibrillation with complete (3rd degree) AV block and inferoposterior STEMI. In the 1980's, it was believed that the right precordial ST depression that frequently accompanies inferior STEMI was due to "anterior subendocardial ischemia." On arrival, here is the ED ECG: No significant change.
Our transport time to the ED was 30 min. Unfortunately, the ED declined as it was viewed as an NSTE. Lake County Ambulance obtained ECG within 9 minutes and transmitted to ED. Serial ECG's obtained, none meeting true STEMI criteria, but dynamic changes noted. We are hopeful for her recovery.
ST-segment Elevation Myocardial Infarction (STEMI) criteria have been the traditional method of cath lab activation. However, patients with occlusions that do not have STE may not activate the system and at least a quarter of the non-STEMI cases have an associated coronary artery occlusion.
However, these figures fail to account for downstream costs due to misdiagnosis, delayed care, or subsequent ED visits. 23 Utilization of terminology, for example, non-emergent, is problematic because field assessment can miss subtleties that ED evaluations catch. ” 31 This term is repeated in the CMS final report on ET3.
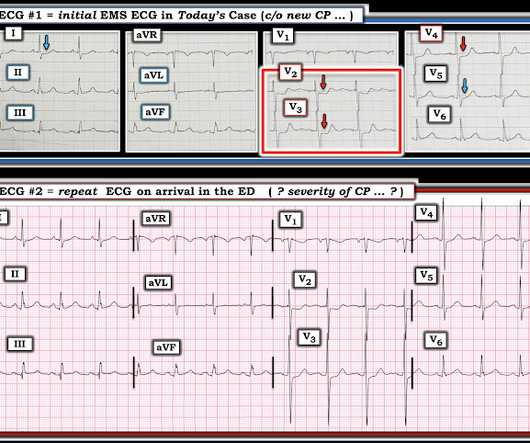
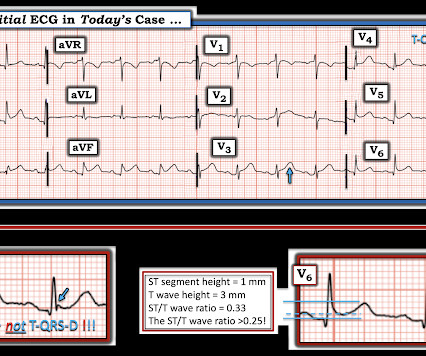
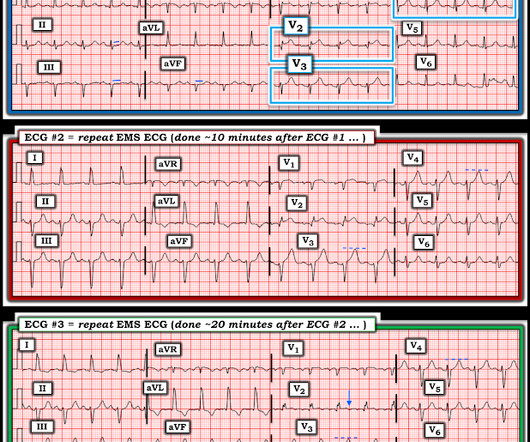
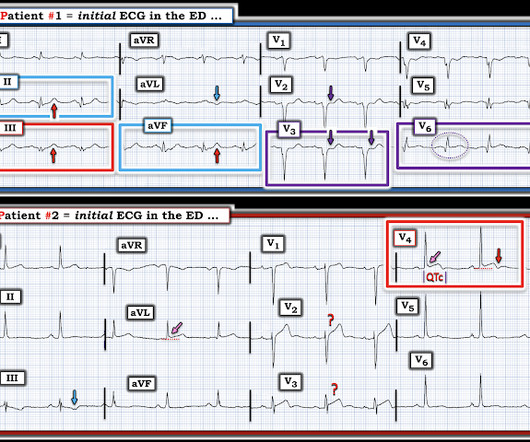
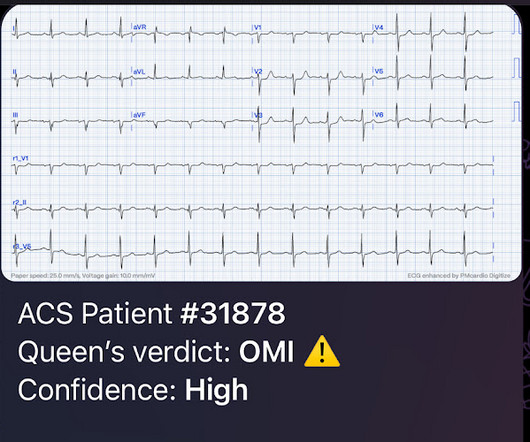
The Zoll algorithm impressively stated: STEMI A paramedic student had the PMCardio AI Queen of Hearts on his phone and this is what it reported: New PMcardio for Individuals App 3.0 Figure-1: Comparison of today's initial EMS ECG — with the repeat ECG on arrival in the ED. Download now for iOS or Android. (Dr.
What could you achieve if you had a patient’s prearrival care information in hand when they arrived at the emergency department (ED)? Repeated medical care because of duplicate records costs over $1,700 per ED visit , while denied claims from patient misidentification cost the average hospital $2.5
Here is his ED ECG: Day 1, "Hampir Stroke," temp 39 degrees : What do you see? There is ST Elevation in V1-V3, but clearly not due to STEMI. He was sure the doctors did not tell him that his brother succumbed to occlusion in the coronary arteries. This is Classic Type I Brugada Morphology.
A prehospital ECG was similar to the first ED ECG, which is shown below. Here is her initial ED 12-lead ECG: There is atrial fibrillation with a rate of approximately 114. Thus, the ACC/AHA 2013 STEMI guidelines now list diffuse ST depression, with ST elevation in aVR, as an indication for thrombolytic therapy. 911 was called.
The emergency department (ED) at Scripps Mercy Hospital San Diego is a different breed of ED. Seeing more than 76,000 annual visits, this urban academic Level I Trauma Center is a STEMI-receiving hospital, geriatric emergency department (GED) certified, and a Stroke Center. Click to enlarge. Click to enlarge. How Do They Do It?
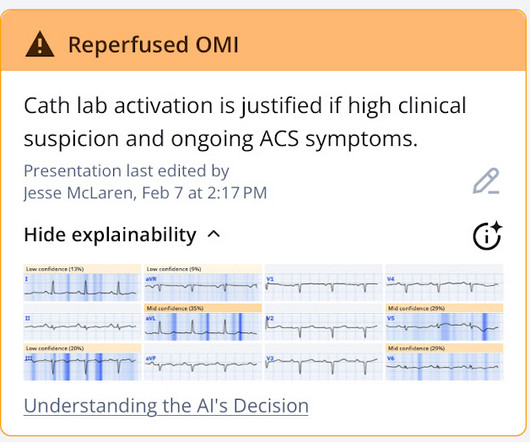
Now as an intern, he is exceptional at EKG interpretation because he was able to learn of the OMI paradigm and importance of pattern recognition before getting poisoned by years of learning STEMI. This is really a transient OMI (or transient STEMI if one uses that terminology and it has diagnostic ST Elevation). The rhythm is sinus.
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis What do you think?
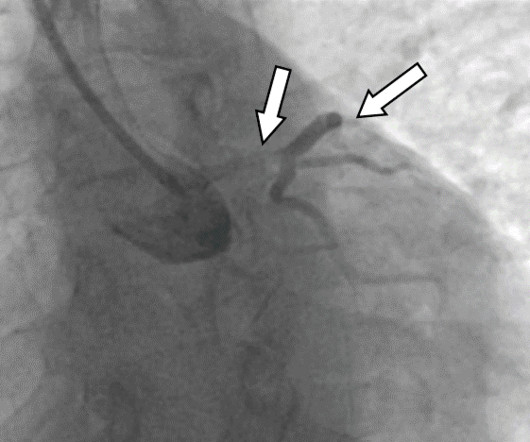
This was interpreted as "inferior STEMI" and the cath lab was activated. Discharge diagnosis was Non-STEMI. The STEMI/NSTEMI dichotomy can make it difficult to identify the culprit lesion, which can be spontaneously reperfused at the time of the angiogram 3. The patient had no further episodes of chest pain.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
Here is his ED ECG (compare with the 2 month previous ECG below it): --Is there a new Q-wave (tiny r-wave) in III? This is almost certainly an acute inferior MI, though does not meet mm "criteria" for STEMI --The beginnings of T-wave inversion suggest an open artery. ng/mL due to the brief RV STEMI. The patient did well.
normal glucose, and mild acute on chronic renal failure (Creatinine from 140 to 170 umol/L), and the following ECG, and they were sent to the ED. The patient was seen three hours later in the ED, with triage vitals showing BP 50 and BP 106/60. ED labs showed a repeat K of 6.6 Labs showed a non-hemolyzed potassium of 6.2,
This was written by Mark Hellerman, Cardiology Fellow at Stony Brook: The Case: A 60 year old man with no reported medical history presents to the ED for evaluation of chest pain. The Case In this case, it is likely that the patient auto-lysed a culprit lesion prior to presentation to the ED.
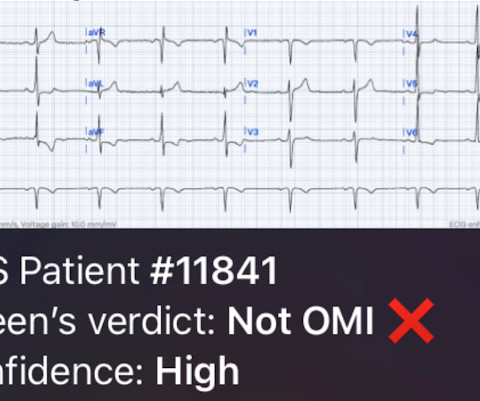
This ECG was recorded 30 minutes later with ongoing pain: Queen of Hearts says no signs of STEMI or Equivalent for both: New PMcardio for Individuals App 3.0 Midwest STEMI Consortium: decreased false positives by 33% (presented at ACC Quality Summit San Antonio 2024) 3. She denied preceding symptoms or recent illnesses.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. This is really good Prehospital, ED, and Cardiolog. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Max Palatnik case Is this Septal STEMI/OMI? Patient with STEMI (-) OMI is now pain free. Five Primary Patterns of Ischemic ST depression, without ST elevation.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Ed Burns (from Life in the Fast Lane) sent me this. See what happens when one fails to diagnose STEMI. Cardiologist declines taking patient to the cath lab.
consult: In summary, this is a 47 year old male with past medical history of CAD s/p STEMI in 2010 s/p PCI to LAD with BMS, HTN, tobacco, alcohol and substance abuse that presented with chest pain and found to have ST elevation with T wave inversion in his ECG. Patient had a negative head CT and was admitted to the ICU for further work-up.
ED echo: The left ventricular ejection fraction appears: Severely reduced No pericardial effusion identified. Remember that 1/3 of MI (both STEMI and NSTEMI) present without chest pain, and that is even more common in women and the elderly. Underlying right basilar atelectasis and or infiltrate cannot be excluded. cm (normal = 0.7
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Emergency (ED placement) Transvenous Pacer appears. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Patient dies. What are your.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Five Primary Patterns of Ischemic ST depression, without ST elevation. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Cardiac Arrest -- Is it STEMI? Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Cardiologist declines taking patient to the cath lab.
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. We looked at 101 STEMI patients from two rural EDs. Date: November 22, 2023 Reference: Stopyra et al.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Cardiac arrest with STEMI pattern: no acute corona. Smith’s ECG Blog and EMCrit Pendell Meyers, MD Scott Weingart, MD, FCCM Stephen S. Patient dies.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
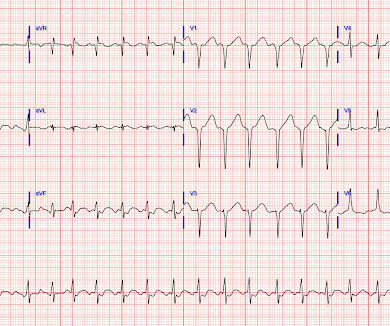
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. Take Home Points Provider assessment of how the patient looks is extremely important.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He wrote most of it and I (Smith) edited.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. The essential "immediate" decision to be made in "zero time" in the ED, is whether or not prompt cath and reperfusion is needed. Could this false positive cath lab activation been prevented?
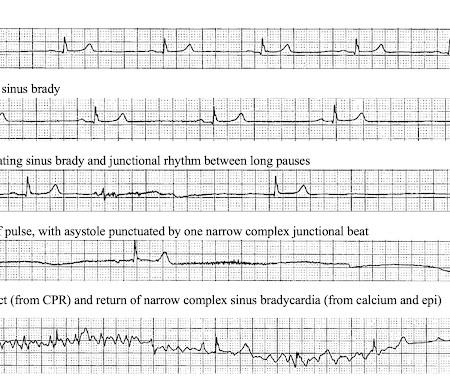
He arrived to the ED with severe hypotension, heart rate in the 70s, unable to follow commands but moving all extremities requiring restraint and sedation, respiratory rate around 24/min being supported with bag valve mask, with significant hypoxemia. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. It’s unclear if the paramedic ECGs were seen or missed in the ED. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. At this point the emergency physician asked for a stat cardiology consult.
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). Despite the ACC guidelines for posterior STEMI, the cardiologist again refused to take the patient to the cath lab. mm STE in the posterior leads.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content