This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Case: You’re doing a ride along with your local emergency medical service (EMS) crews and responding to an out-of-hospital cardiac arrest (OHCA). The paramedic is trying to get intravenous (IV) access to give epinephrine per the protocol. Epinephrine has long been a cornerstone in the management of OHCA.
Murphy JD, MS, PA-C, EFO 5 min read Share To: Shutterstock/Fineart1 Emergency medical services (EMS) are essential in delivering timely care during medical crises. As technology evolves, EMS systems are undergoing a transformative shift toward automation.
Emergency medical services(EMS) has historically been a punitive system, resulting in people being unforthcoming about issues or concealing minor infractions in hopes of evading discipline. Scenario One A paramedic forgets to restock epinephrine 1:1,000 in the medical bag, and the next crew responds to an anaphylaxis call without it.
Originally published at The Pediatric EMS Podcast on March 5, 2035. This is the Pediatric EMS Podcast with the mission to provide case-based discussion with evidence-based recommendations by content experts in prehospital pediatric medicine in order to advance the care of children outside the hospital. Reposted with permission.
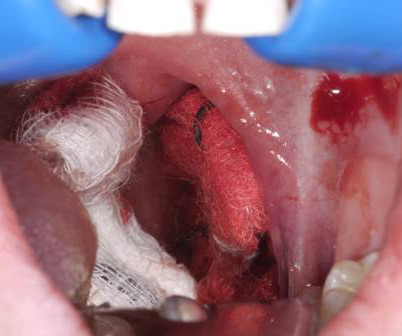
6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention. 7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression.
This observational study aims to describe the usage of vasopressors by EMS, and to assess how vasopressor usage differs between transport and hospital environments. Epinephrine was administered to 163 (13.4%) patients. In total, 505 (41.7%) of patients received multiple vasopressors during EMS transport.
In the most recent BroomeDocs podcast, we talk about an attempt to use the IM route to give cardiac arrest victims epinephrine faster. The podcast and Research Roundups blog post might actually come out next week.)
EMS administrators and hospital logistics teams should consider how integrating drone delivery can complement existing workflows. For EMS chiefs and emergency logistics managers, staying informed and preparing for these regulatory changes now will offer a strategic advantage.
WE, AS EMS PROFESSIONALS, SHALL PROVIDE COMPASSIONATE, APPROPRIATE CARE TO ALL PATIENTS. EMS must rely on the hazmat team to monitor the air and not rely on their sense of smell. Children who develop stridor may be treated with racemic epinephrine (0.25- 0.75ml of 2.25% racemic epinephrine to 2.5
Yet at the same time, despite a large-scale Holmberg study involving over 6,000 patients suggesting potential harm, epinephrine remained part of the pediatric symptomatic bradycardia protocol. EMS is a unique subspecialty within medicine, and we owe it to our patientsand to ourselvesto dig deeper. By now, you can see the pattern.
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
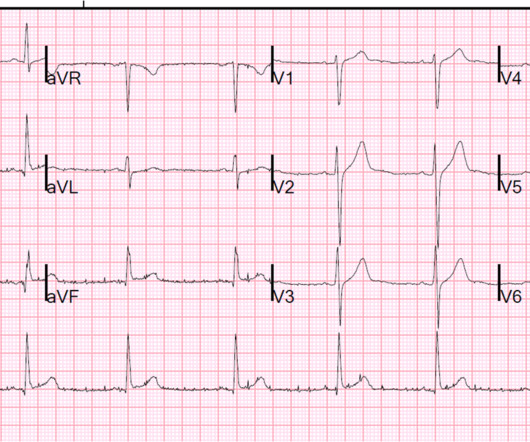
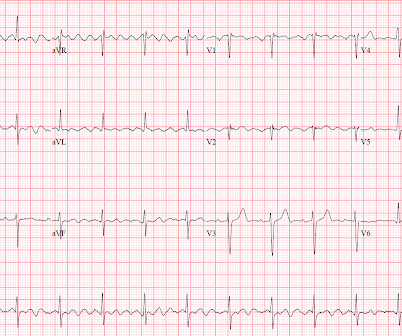
Authors: Lloyd Tannenbaum, MD (EM Attending Physician, APD, Geisinger Wyoming Valley, PA); Christian Daniello, MD (Staff Physician, Geisinger Wyoming Valley) // Reviewer: Brit Long, MD (@long_brit) Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations.
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Controversies and Consensus in EM. Post the new article about coronary occlusion Great dynamic BTWI case dunbar extreme subtle inferior MI Aug 13 iMessage, Sudden weakness with bradycardia and bizarre T-waves 1304490 old vs. new anterior MI, with video, lead. Beware Automated Interpretations of Atrial Fibrill. Sept 20-22 Nor.
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Hyperkalemia paper from West J EM Great V FIb Arrest Case type II STEMI, hypoK 3.3 A 50-something with chest pain and minimal precord. Chest pain and precordial ST depression which reso. Wide Complex Tachycardia: is the patient stable or. The risk of myocardial rupture 15 hours of chest pain. Too late for thrombolytics.
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Texted from a former EM resident: 70 yo with synco. LBBB wellens mimic, trops neg, resolves, then APTA Subacute LAD OMI images in file - first ECG was no. How a pause can cause cardiac arrest Recurrent syncope. Diagnosis made after 20 years o. Acute chest pain, right bundle branch block, no ST.
Controversies and Consensus in EM. Post the new article about coronary occlusion Great dynamic BTWI case dunbar extreme subtle inferior MI Aug 13 iMessage, Sudden weakness with bradycardia and bizarre T-waves 1304490 old vs. new anterior MI, with video, lead. Beware Automated Interpretations of Atrial Fibrill. Sept 20-22 Nor.
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
Wang (21) Dressler's syndrome (2) Drug Effect (2) Dual AV nodal pathways (6) Dynamic T-waves (10) ECG Radiologist (1) ECG misdiagnosis (2) ECLS -- Extracorporeal Life Support (1) ECMO -- Extracorporeal Membrane Oxygenation (3) EMS voltage cutoff (2) EP study (1) ESRD (1) Early Intervention for NonSTEMI (3) Early Repol Inferior and Lateral (1) Early (..)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content