This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
These systems use real-time data from electronic health records (EHRs) and other sources to predict which patients are at risk of adverse outcomes, such as cardiac arrest or transfer to an intensive care unit (ICU) [1.2]. Despite the potential benefits, integrating AI into clinical workflows presents challenges.
Supportive Care Intensive monitoring, often in an ICU setting. Types of Necrotizing Fasciitis Type I (Polymicrobial) Involves aerobic and anaerobic organisms (e.g., Bacteroides, Clostridium, Peptostreptococcus). Common in immunocompromised patients or those with comorbidities (e.g., diabetes, peripheral vascular disease).
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
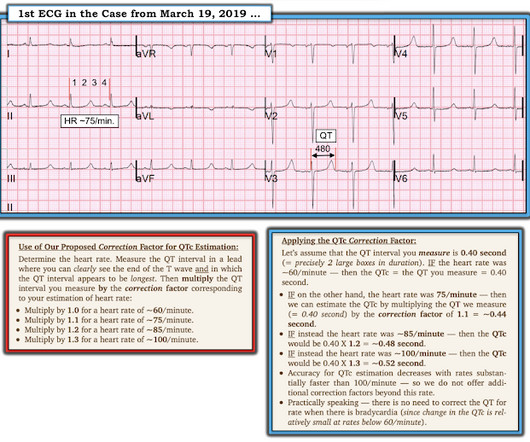
CASE CONTINUED She was admitted to the ICU. T-waves are quite tall and possibly peaked (HyperK?), but potassium returned normal. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis. What is the QT interval? Bogossian et al. (1)
A large observational study of > 2000 patients found an association with fever at presentation and ICU survival for patients with severe sepsis or septic shock ( Sunden-Culberg 2017 ). Fever in the Emergency Department predicts survival of patients with severe sepsis and septic shock admitted to the ICU. Sat 93% on RA.
Restriction of intravenous fluid in ICU patients with septic shock. Both studies demonstrated no difference in their primary outcome of mortality before discharge home by day 90 when employing a ‘liberal’ or ‘restrictive’ approach to fluid resuscitation for patients in septic shock. Crit Care Med. 2021;49(11). N Engl J Med. N Engl J Med.
The patient is admitted to the ICU and slowly improves over time. Doppler study of portal vein and renal venous velocity predict the appropriate fluid response to diuretic in ICU: a prospective observational echocardiographic evaluation. Utilizing color doppler, you want to try to identify the interlobar vessels within the parenchyma.
Early bolus epinephrine administration during pediatric cardiopulmonary resuscitation for bradycardia with poor perfusion: an ICU-resuscitation study. This moment is more than just a guideline change—it’s a validation of the relentless pursuit of evidence over tradition. Resuscitation. 2020;149:200–207. doi:10.1016/j.resuscitation.2019.12.032
My goal in this column is to share tips, tricks, and emerging concepts from the intensive care unit (ICU) that you can use on your next shift in the emergency department (ED). Known hypotension, as a bridge to a continuous infusion of a pressor. Using push-dose pressors can be your lifeline while waiting for the infusion bag to arrive.
fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
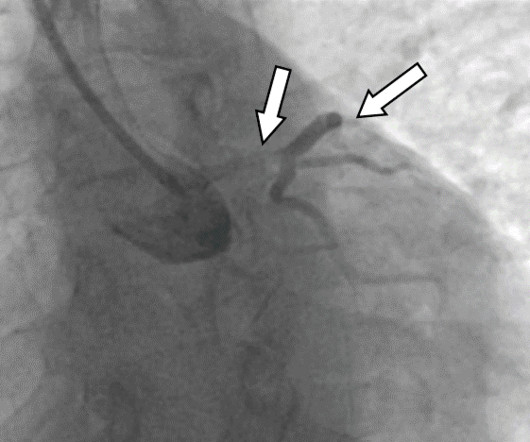
Pt was extubated a day later and continues her recovery in the ICU. Pt had thrombotic nearly occlusive LM lesion with TIMI 1 flow in the LAD, Ramus, and Left Circumflex, and she was transferred for emergency CABG x 3. Etiology possible thromboembolic and less likely due to atherosclerosis or plaque rupture. We are hopeful for her recovery.
Intubation performed in all settings (out-of-hospital, emergency department, ICU, and operating room). Clinically Diverse Patient Population : The study included patients from varied clinical settings (ED, ICU, OR, and pre-hospital). Randomized controlled trials or comparative non-randomized observational studies. airway scope).
The characteristics that were significantly different between the LR and NS exposure groups race, organ dysfunction at presentation, ICU admission, hemoglobin SS genotype, discharge year, and hydroxyurea use were appropriately included as confounders in the TMLE analysis.
Clarke took from 19781980 provide a glimpse into working in an emergency department in the years the specialty was being established. At first glance, one might notice the clothesnurses in white dresses and doctors in wide ties or bellbottom jeansor the hairafros, sideburns, and mustaches aplenty. Now, we have ultrasound or CT scans to confirm.
After managing her sepsis, her oxygenation remains poor, with saturations in the 88-92% range despite supplemental oxygen via a nonrebreather mask, and she now shows signs of worsening fatigue. Exclusions: Studies involving reviews, conference abstracts, case reports, or lacking full text. strategies.
Welcome to the first episode of the Broomedocs podcast for 2025. Justin and I are back for more nerdy goodness to make you smarter in the Resus room, or at a pub trivia night more likley… wether it is about salt correction, dissection or infection we can help you out! Listen in and learn! Dimer is useful in the low risk group. Emerg Med J.
Background: Patients with sepsis are routinely treated with empiric broad-spectrum antibiotics while awaiting source identification, as recommended by the surviving sepsis campaign.2 2 Vancomycin, in combination with either piperacillin-tazobactam or cefepime, is commonly used for empiric treatment in these cases. In 2021, Buckley et.
History of Present Illness The collateral history indicates that her symptoms began one week into her journey, but medical care was inaccessible at the time. The family reports no history of food allergies, insect bites, or contact with sick individuals. The patient did not receive pre-travel prophylaxis for malaria, hepatitis A, or yellow fever.
Effectiveness of Nasal High-Flow Oxygen during apnoea on Hypoxaemia and Intubation Success in Paediatric Emergency and ICU Settings: a randomised, controlled, open-label trial. Thats exactly what Shane George et al. George S, Williams T, Humphreys S, et al. Lancet Respiratory Medicine.
We discuss the basics of EEG in the ICU, including when to do it, selecting the appropriate study, and the basics of bedside interpretation, with Carolina B Maciel, MD, MSCR, FAAN, triple boarded in neurology, neurocritical care, and critical care EEG. Learn more at the Intensive Care Academy! Find us on Patreon here! Find us on Patreon here!
In humans, its pharmacologic relative dexmedetomidine is used for procedural sedation and ICU management, but medetomidine itself has no approved human indication. Medetomidine is a central alpha-2 adrenergic agonist used in veterinary medicine to induce sedation and analgesia. 2 Withdrawal from medetomidine presents a different challenge.
Skip to content Twitter Google+ Facebook Reddit RSS The Bottom Line A compendium of critical appraisals in Intensive Care Medicine research and related specialties Home About Us Summaries Intensive Care Medicine Emergency Medicine Peri-operative Medicine Blog News EBM Editorial Submit a review Wessex ICS You are here: Home Blog Critical Care Evidence (..)
Lower intubation, need for BPAP and ICU admission in bolus group (Levy 2007). SCAPE differs in several significant ways: rapid onset (hours), respiratory distress, severe HTN, may or may not be systemically volume overload. Meta-analyses demonstrate reduced need for intubation, improved survival, improved respiratory indices (e.g.,
1 Three small noninferiority RCTs suggested that 7 days of antibiotics may be sufficient for patients with gram-negative bacteremiabut these trials had notable limitations: they excluded ICU patients, included only clinically improving individuals, and did not assess gram-positive infections. male Setting at enrollment: ICU: 55.0%
Value-Based Care in Emergency Medicine The transition to value-based care has been slower than anticipated, particularly for specialties like emergency medicine that need more predefined patient populations or well-defined episodes of care. However, emergency physicians have made significant strides in recent years. No external validation.
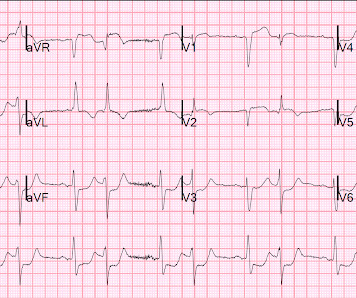
She was admitted to the ICU on an amiodarone drip and continued to improve. Here is her initial ED 12-lead ECG: There is atrial fibrillation with a rate of approximately 114. There is extreme ST depression in multiple leads and ST elevation in aVR, suggesting left main and/or 3 vessel disease ischemia. Is this Acute Coronary Syndrome?
Throughout her career as a pharmacist, Jennifer Esch, PharmD, MBA, BCPS, has worked in a variety of hospital settings from the ICU to the emergency department. This series highlights members of the GEDC community who are clinical champions for older adults in the emergency department. That was a whole lot better than I expected,” Esch said.
PMID: 40378193 #2: OPTPRESS – High MAP Goal in Older Patients with Septic Shock Spoon Feed — This randomized control trial of older ICU patients with septic shock in Japan showed higher mortality and more frequent adverse events in patients randomized to a high MAP goal (80-85 mmHg) compared to usual care (65-70 mmHg). Clin Infect Dis.
9 Consider ICU if related to thyrotoxicosis as these patients require monitoring for cardiac arrhythmias. Hip flexion ⅖ bilaterally, knee extension ⅗ bilaterally, plantar and dorsiflexion ⅘. Bilateral upper extremities shoulder flexion, elbow flexion, and extension 5/5. MSK: no rashes or lesions appreciated. mEq/L Magnesium: 1.33
Recognize pulmonary-renal syndromes early. Initiate high-dose steroids immediately for unstable patients without waiting for ANCA results. GPA is rare but life-threatening – early recognition saves lives.
Tight Blood-Glucose Control without Early Parenteral Nutrition in the ICU Gunst et al. N Engl J Med 2023;389:1180-1190 DOI: 10.1056/NEJMoa2304855 Clinical Question In ICU patients not receiving early parenteral nutrition, does liberal glucose control (initiating insulin when blood glucose level [BGL] >11.9 to 6.1 […]
She is intubated, resuscitated and admitted to the ICU. An abdominal CT is ordered, during which the patient vomits, aspirates, develops bradycardia and has a PEA cardiac arrest. The non-contrast CT scan shows a very large, distended fluid-filled stomach above the diaphragm suggesting the presence of a gastric volvulus.
On physical exam, the patient is lethargic, has nasal flaring, and is using accessory muscles to breathe. Lung sounds are clear. On cardiac exam, there is normal rate and rhythm without murmur, rubs, or gallops. His capillary refill is 2 seconds. His surgical incision looks clean and without any signs of infection.
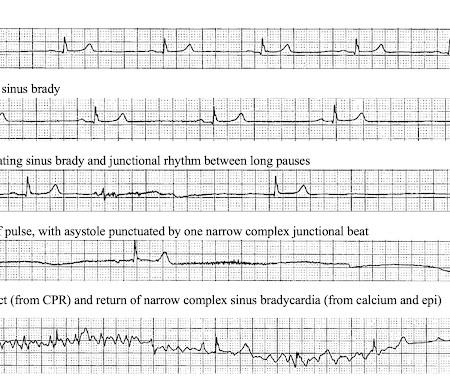
and the patient was given more insulin/dextrose/calcium and admitted to ICU. Two hours later the patient became somnolent and the monitor showed the following rapid changes: ECG after ROSC Repeat K was 6.4 A good reminder of recommendations for calcium for either K>6 with any ECG changes (when the patient was first seen) or K>6.5
Children without vomiting within 6 hours of iron ingestion will almost never have significant toxic effects. 6 Can see subsequent electrolyte disturbances and dehydration related to severity of GI symptoms. In severe toxicity, hematemesis, melena, or hematochezia may occur. Be wary of this stage. This stage does not always occur. 2 L/hr in adults.
Can be a smoldering infection in patients with immunocompromising conditions. Consider cryptococcus meningitis in these patients. Recommended testing: Serum lab tests are commonly obtained, but they are not helpful in ruling in or out bacterial meningitis. Cerebrospinal fluid analysis (ideally within 1 hour of presentation to ED) is necessary.
Octreotide is not the treatment of choice for HRS in the ICU; use norepinephrine and titrate up until you see an increase in urine output (or it doesn’t work). Terlipressin works too but is pricey and more appropriate for outside the ICU. Terlipressin works too but is pricey and more appropriate for outside the ICU.
The ICU team comes down and rapidly admits the patient. The GI team is standing by in the ICU ready to do an emergent scope. The patient’s initial high sensitivity troponin was 7 ng/L and was trended by the ICU team upstairs. He was so weak that we had to carry him out of the bathroom and then sprinted over here. Any ideas?”
Intubated patients in the ED should have soft, wrist restraints places without the need for arduous, high-risk documentation or sitters Intubation Checklist EMCrit 176 – Updated EMCrit Rapid Sequence Intubation Checklist Awareness during Paralysis EMCrit 331 – Awareness after Resus RSI and ICU Paralysis – It is Unacceptable!!!
Today we'll walk through some interesting bits of the new IDSA/SCCM guideline on evaluation of new fever in the adult ICU patient (available free here). how should temperature be evaluated? This is frankly a mess. Bladder catheter or esophageal probe are best, but usually not used.
Caleb Lin Hyperbaric Oxygen for the ICU Patient OVERVIEW INTENSIVE CARE INDICATIONS PRACTICAL ISSUES IN CRITICAL CARE Consideration & Prior to Treatment In the Chamber A: ETT cuff to be filled with sterile water or connected to dynamic cuff inflator B: Titrate ventilation to PaCO2, note that EtCO2 is not linearly proportionate at higher pressures (..)
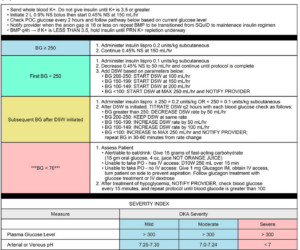
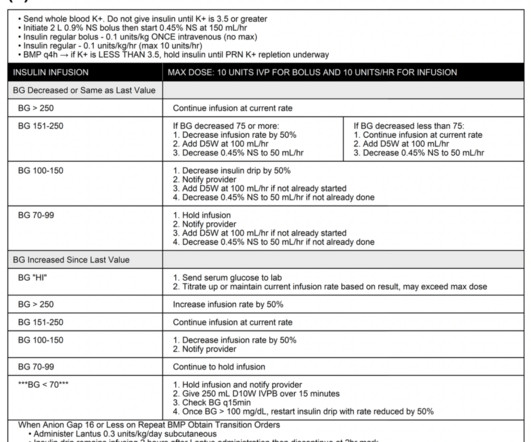
The standard of care of treating DKA is fluid resuscitation, electrolyte management, and intravenous insulin infusion in the intensive care unit (ICU) setting for close glucose and electrolyte monitoring. Recent research aims at investigating the treatment of DKA with subcutaneous insulin in non-ICU settings. Image from cited article.
The patient states he has had multiple “diabetic emergencies” in the past and usually ends up in the intensive care unit (ICU) on a drip. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?” However, the ICU is full and the patient will likely be boarding in your ED for a bit before coming upstairs.
He is board certified […] The post SGEM#368: Just A Normal Saline Day in the ICU – The PLUS Study first appeared on The Skeptics Guide to Emergency Medicine. Then, the BaSICS trial (a multicentred RCT done in 75 Brazilian ICUs) came along and compared saline to Plasma-Lyte at what the authors deemed slow and fast infusion rates.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content