This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
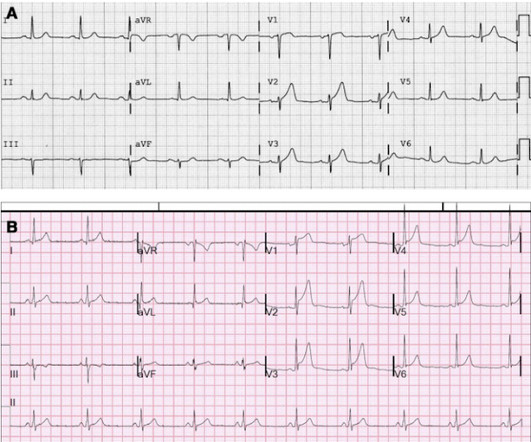
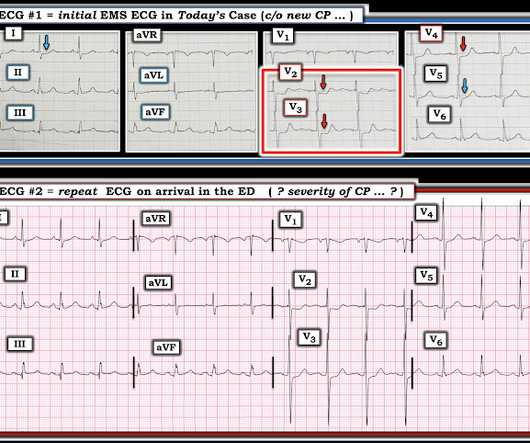
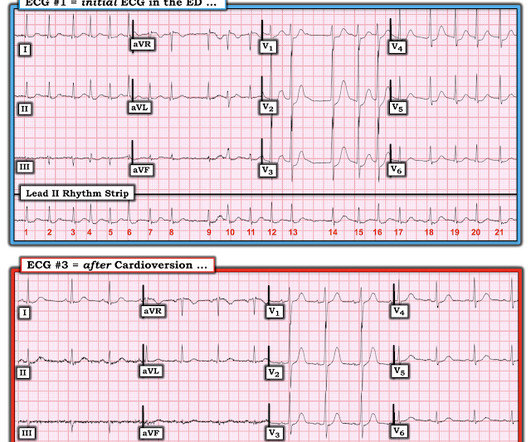
interesting spontaneous reperfusion case 1413140 prehospital STEMI first ED ECG is here, with 3/10 pain: But this is the same patient just 10 minutes before, with 7/10 pain Isn't it ridiculous to say that the patient has both a STEMI and an NSTEMI? ACS is dynamic. It can't be given one static name. Now the patient has one disease: OMI.
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria.
For instance, there was no protocol for stroke or STEMI. At some point along the way we had protocols for spinal motion restriction, alcohol withdrawal, stroke and STEMI, CPAP, and termination of cardiac arrest resuscitation on scene. There were fewer than 50 protocols in the book, along with pages for 24 medications and 8 procedures.
The subsequent diagnosis of an ST-segment elevation myocardial infarction (STEMI) sets forth a cascade of events that typically culminates in the patient being transported to hospital capable of emergent percutaneous coronary intervention (PCI). However, the notion of “STEMI equivalents” has gained traction.
Diagnosis: Atrial Fibrillation with complete (3rd degree) AV block and inferoposterior STEMI. In the 1980's, it was believed that the right precordial ST depression that frequently accompanies inferior STEMI was due to "anterior subendocardial ischemia." Heart block in inferior STEMI is due to ischemia of the AV node.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. However, many patients with de Winter ECG pattern have TIMI 0 at angiography and the ECG pattern does not necessarily progress to STEMI. 17 have HATW. Under Review.
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. Another EKG was also obtained. Very early in the morning, he reported recurrence of a heartburn sensation, so another EKG was obtained.
But if there’s natural ST segment elevation and depressions all over a left bundle branch block, how do we know when a patient is having a STEMI or not? Notice how the QRS complex have a very high voltage and the ST segments are appropriately elevated or depressed in the opposite direction of the QRS complexes (more on this below).
His initial EKG is the following: What do you think? Naturally you would assume that this was a large, multicenter trial, right? This was based on 11, thats not a typo, ELEVEN patients. Ok, so what did the PROCAMIO trial find? Ok, so what did the PROCAMIO trial find? Well, the trial was a multicenter prospective open label trial.
Serial ECG's obtained, none meeting true STEMI criteria, but dynamic changes noted. The STEMI alert to OR prep time for CABG was around 60 minutes and this exemplifies excellent, expedient teamwork. I'll continue studying OMI / NOMI in ECGs and use the QOH to better provide patient care in the prehospital setting.
Uh, Rate, rhythm, uhhh STEMI? Another great shift with that jackass attending who refuses to learn any of the interns names. I love residency training, you think to yourself. Ill take a closer look at Mr. Deltars ECG. Is that how I read them? you ask, still not completely focused. Ok, better than expected, Mr. Bigshot.
Would you believe that once upon a time in Connecticut, STEMIs were brought to the closest hospital regardless of capability.” They were still brought to the closest hospital rather than a thrombectomy capable hospital and I was saying this really should be changed like we changed the system for trauma and STEMIs. Again, true.
The median time between emergency call and thoracotomy was 22 (17-29) minutes. The underlying cause of the TCA was cardiac tamponade in 105 patients (18%), exsanguination in 418 patients (70%), or a combination of both in 72 patients (12%). for all other causes). The duration of TCA was also associated with survival (16% for 10 minutes).
While this mechanism has enabled states to draw down billions in additional federal funds, CMS argues that it distorts the fiscal integrity of Medicaid by allowing states to effectively cycle federal dollars back to providers without a commensurate state contribution or measurable expansion of care for enrollees.
It is tempting to say that the ST depression was "posterior STEMI" on these initial ECGs, but that is not so. The ST depression was not V1-V3 (as in posterior STEMI), but rather V3-V6 (which is what is seen in subendocardial ischemia). Comment 2: This is a great example of how the dichotomy between STEMI and Non-STEMI is false.
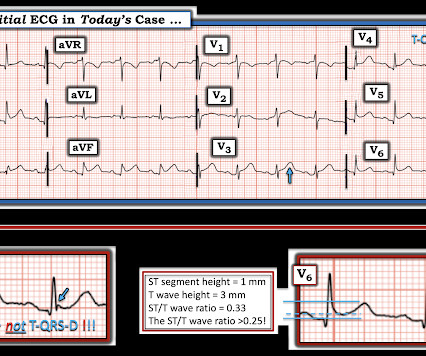
The Zoll algorithm impressively stated: STEMI A paramedic student had the PMCardio AI Queen of Hearts on his phone and this is what it reported: New PMcardio for Individuals App 3.0 There is a hyperacute T-wave in V6, which is the lateral part of the posterior wall and a common supportive finding in posterior OMI. Is this OMI?
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Inferior STEMI with AV Block, Cardiogenic Shock an. The QRS proves it. Posted by Steve Smith at 6:29 AM Email This BlogThis! Patient dies. Atrial Fib with RVR.
There is ST Elevation in V1-V3, but clearly not due to STEMI. Here is his ED ECG: Day 1, "Hampir Stroke," temp 39 degrees : What do you see? This is Classic Type I Brugada Morphology. The patient may have been experiencing episodes of polymorphic VT. Here are the ECG criteria for Brugada pattern.
Thus, the ACC/AHA 2013 STEMI guidelines now list diffuse ST depression, with ST elevation in aVR, as an indication for thrombolytic therapy. Here is her initial ED 12-lead ECG: There is atrial fibrillation with a rate of approximately 114. There is some STE in V1 and aVL, further suggesting left main involvement.
ECG B shows you some abnormal looking T waves that don’t meet STEMI criteria. Finally, ECG C shows an anterior STEMI! ” “Correct. All the other attendings would let me discharge him.” Young one, come over here, let’s look over this ECG together and then maybe you’ll understand where I’m coming from.” V2 and V3 look biphasic.
The PMCardio Queen of Hearts app asks you, before giving an interpretation of OMI ("STEMI-Equivalent"), whether the patient's clinical presentation is high risk for OMI. Dizziness is so unlikely to be OMI without an obvious ECG, that I am going to pretend that this patient presented with chest pain. So let's pretend this is acute chest pain.
A prehospital ECG showed ST Depression in V1-V3 and the medics were concerned for posterior STEMI. Charts showed a history of some mitral regurgitation and an enlarge left atrium, as well as hypertension treated with a thiazide diuretic. Pulse was 128 and irregular, BP was 141/75. How do we make the distinction?
Now as an intern, he is exceptional at EKG interpretation because he was able to learn of the OMI paradigm and importance of pattern recognition before getting poisoned by years of learning STEMI. This is really a transient OMI (or transient STEMI if one uses that terminology and it has diagnostic ST Elevation).
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI. Mostly the same findings and reasoning as the current ECG.
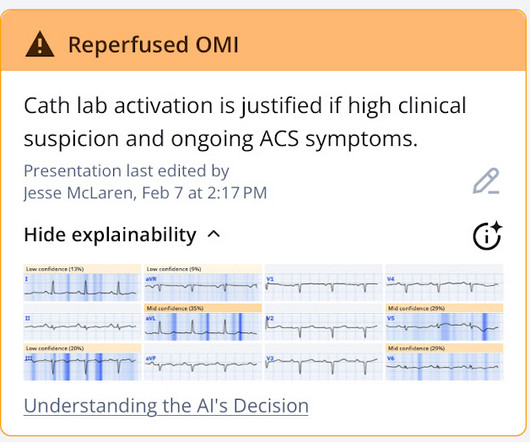
This was interpreted as "inferior STEMI" and the cath lab was activated. Discharge diagnosis was Non-STEMI. The STEMI/NSTEMI dichotomy can make it difficult to identify the culprit lesion, which can be spontaneously reperfused at the time of the angiogram 3. NSTEMI or reperfused OMI? So which was the culprit?
Seeing more than 76,000 annual visits, this urban academic Level I Trauma Center is a STEMI-receiving hospital, geriatric emergency department (GED) certified, and a Stroke Center. During my visit the greeter area was quiet, uncluttered, and virtually empty at 4 p.m. Other operating characteristics for this department are seen in Table 1.
The differential is: 1) LAD occlusion proximal to the septal perforator with wraparound to inferior wall (that much STE in V1 is quite specific for septal involvement with anterior STEMI) vs. 2) Proximal RCA with RV involvement. Is it important to know whether this is LAD or RCA? Somewhat, but not hugely important. First, the 12-lead: 1.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
Acute Intraoperative STEMI in a Toddler. We suggest that this list can help you discover relevant or interesting articles for your local journal club or keep you up to date on the latest paediatric research. For some of us, the summer holidays are approaching, a time for relaxation and re-charging of the mental batteries. Rienvichit P, et al.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! A good reminder of recommendations for calcium for either K>6 with any ECG changes (when the patient was first seen) or K>6.5 Hyperkalemia requires calcium if >6.5
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. A Middle-Aged male with Chest Pain and an Unusual ECG Doctor, should we activate the hospital's "STEMI a. Disclaimer Cases come from all over the world.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. hours of chest pain Chest Pain and Right Bundle Branch Block Is this acute STEMI? Is this inferor STEMI? Disclaimer Cases come from all over the world. Patient dies.
Importantly, one trial of 925 consecutive STEMI-positive occlusion myocardial infarctions found that 26% had presentation troponin values < 99th percentile when then presented less than 2 hours from symptom onset and 14% had values < 99th percentile when they presented with symptoms for greater than 2 hours.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Severe RVH with large RV on echo, not a PE "I have food poisoning" Article on STEMI vs. BER Why is there ST depression in aVL in this case of. Patient dies.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. The delay between OMI and STEMI claims yet another. Brugada with superimposed anterior STEMI Chest pain. Disclaimer Cases come from all over the world. What is it??
This ECG was recorded 30 minutes later with ongoing pain: Queen of Hearts says no signs of STEMI or Equivalent for both: New PMcardio for Individuals App 3.0 This ECG was recorded 30 minutes later with ongoing pain: Queen of Hearts says no signs of STEMI or Equivalent for both: New PMcardio for Individuals App 3.0 Willy Frick, from St.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Updated 1 hour lecture: The False STEMI-NonSTEMI D. Disclaimer Cases come from all over the world. Five Primary Patterns of Ischemic ST depression, without ST elevation.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. A very fast narrow complex tachycardia in an Infant Do patients with LBBB and STEMI, when reperfused, awesome repost: repost: [link] Rick Abbott case DSECGB: ST resolution.
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Sunday, August 25, 2013 Anterior ST Elevation - Is it STEMI?
How well does the computer interpretation perform? -- in this case, the computer diagnosed STEMI but the patient had Fever with Brugada -- A young F is hyperthermic, delirious, and dry: Fever-induced Brugada? A 50-something male presented to triage with chest pain for one day. There is an rSR' in lead V1 without any spike of the R'-wave.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Disclaimer Cases come from all over the world. Patient identifiers have been redacted or patient consent has been obtained. Cardiologist declines taking patient to the cath lab.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Disclaimer Cases come from all over the world. Patient identifiers have been redacted or patient consent has been obtained. Cardiologist declines taking patient to the cath lab.
Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Disclaimer Cases come from all over the world. Patient identifiers have been redacted or patient consent has been obtained. Cardiologist declines taking patient to the cath lab.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content