This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Long and Koyfman (3) wrote up an excellent review article looking at multiple trials trying to figure out what medication would be best (if any) for the treatment of stable monomorphic ventricular tachycardia. His initial EKG is the following: What do you think? So, we should always use procainamide, right?
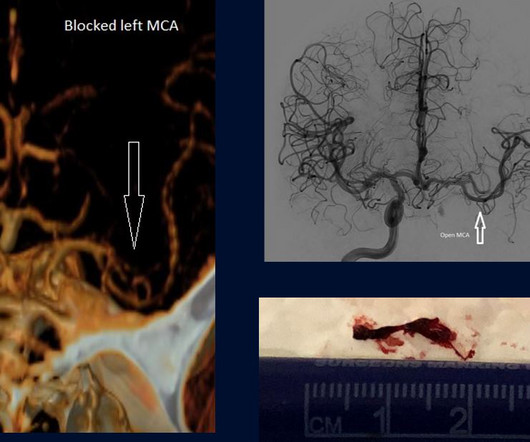
Would you believe that once upon a time in Connecticut, STEMIs were brought to the closest hospital regardless of capability.” They were still brought to the closest hospital rather than a thrombectomy capable hospital and I was saying this really should be changed like we changed the system for trauma and STEMIs. Again, true.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. The QRS proves it. Patient dies.
I reference that article in my book chapter on postinfarction pericarditis and myocardial rupture. See these two articles: This one shows an example ECG: [link] This one compared AMI patients with and without rupture. That is true (but incidence was only 3.4% More importantly, they did not look at the ECGs.
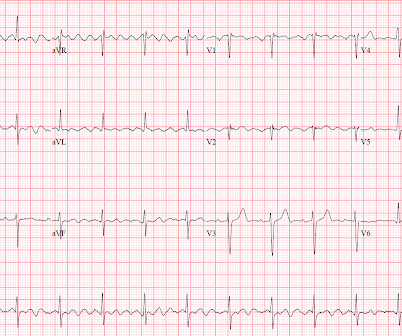
ECG B shows you some abnormal looking T waves that don’t meet STEMI criteria. Finally, ECG C shows an anterior STEMI! ” “Correct. V2 and V3 look biphasic. Now let me tell you about this patient. And in Type B you see broad, symmetric, inverted T waves, often seen in V1-V4.” Type B is more common than Type A.
Now as an intern, he is exceptional at EKG interpretation because he was able to learn of the OMI paradigm and importance of pattern recognition before getting poisoned by years of learning STEMI. This is really a transient OMI (or transient STEMI if one uses that terminology and it has diagnostic ST Elevation). Do not Wait!!
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI. Mostly the same findings and reasoning as the current ECG.
Seeing more than 76,000 annual visits, this urban academic Level I Trauma Center is a STEMI-receiving hospital, geriatric emergency department (GED) certified, and a Stroke Center. She has written articles and books on ED quality, safety, and efficiency. Other operating characteristics for this department are seen in Table 1.
We suggest that this list can help you discover relevant or interesting articles for your local journal club or keep you up to date on the latest paediatric research. Reviews and opinion articles Exception From Informed Consent in Pediatric Trials. Acute Intraoperative STEMI in a Toddler. We hope that you enjoy the list!
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. Is this inferor STEMI?
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
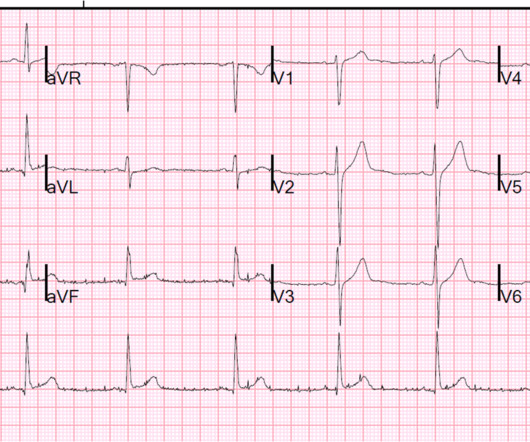
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Sunday, August 25, 2013 Anterior ST Elevation - Is it STEMI?
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
Dr. Smiths Google Scholar Profile Dr. Smith Articles on PubMed This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 Some are STEMI-equivalents. Here are some basic concepts before we get into the ECGs: STEMI and NonSTEMI are arbitrary terms that may confuse the clinician. International License.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content