This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
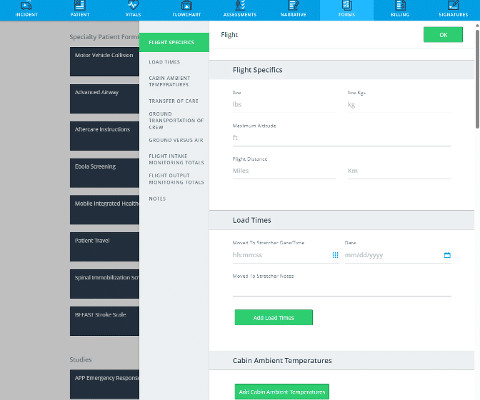
Were making the jump to general availability (GA) and adding new features such as CAD and Cardiac Monitor integrations, Longitudinal Record (LR), and Mobile-to-Mobile functionality. This basic version will not include auto-import configuration, and integrations with CAD and EHR will not be added until upcoming releases in 2025.
In my experience — even when everything points to Stress Cardiomyopathy — it is not always possible to rule out concomitant severe CAD, or even ACS. I favor doing some sort of coronary artery imaging for patients suspected of having Takotsubo if the coronary arteries have not been imaged previously.
A 41-year-old South Asian male with history of hypertension, alcohol use disorder and hyperlipidemia, who has a strong family history of CAD presented with central substernal burning, pressure, and pain with associated diaphoresis.
Because if such severe CAD is present, the patient is likely to need CABG. They show that if there is not >/= 1 mm STE in aVR, then ACS is highly unlikely to be due to severe 3-Vessel disease or Left Main. why is this important? If they need CABG, then the surgeon will usually be unhappy if the patient received clopidogrel.
A patient with history of severe CAD, CABG, with all native vessels occluded, on maximal medical therapy presented with his typical angina. NSTEMI: Patient with known severe CAD presenting with troponin elevation up to 21 and chest pain that was refractory to initial nitroglycerin therapy suggestive of unstable angina.
consult: In summary, this is a 47 year old male with past medical history of CAD s/p STEMI in 2010 s/p PCI to LAD with BMS, HTN, tobacco, alcohol and substance abuse that presented with chest pain and found to have ST elevation with T wave inversion in his ECG. Patient had blood cultures drawn.
EKGs on phone from 12/24 Next morning: Patient with DM-II, HTN, recent stressful circumstance presented with typical chest pain and found to have elevated troponin and significant inferolateral ST elevation which prompted cath lab activation but coronary angiogram showed no obstructive CAD. TTE with lateral WMA and reduced EF. LMCA: Normal.
Angiogram The patient did go for an angiogram and there was no occlusion present, and no definite culprit, although there was diffuse CAD and one possible culprit: "There is a medium-large caliber OM3 with 40-50% stenosis in the mid-segment and lumen irregularity that could suggest dissection or plaque rupture, but TIMI III flow throughout."
Multivessel CAD 2. The calculated post stress ejection fraction is 44%. Inferolateral/anterolateral/inferior akinesis noted. EKG reveals marked ST segment depression at rest and following stress. Cardiology consult impression 1. Ischemic cardiomyopathy, EF 45 --> 20% 3.
He denied any known history of CAD, but did report ASCVD risk factors to include HTN, HLD, and DM. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. The VT vs SVT with Aberrancy debate is beyond the scope of this particular blog post. Here is the ECG after 200J. Examples provided below.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Edited by Smith He also sent me this great case.
Patient 2 A man in his 50s with history of CAD and prior PCI, diabetes, presented with acute constant chest pain for the past few hours. Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. He was discharged home.
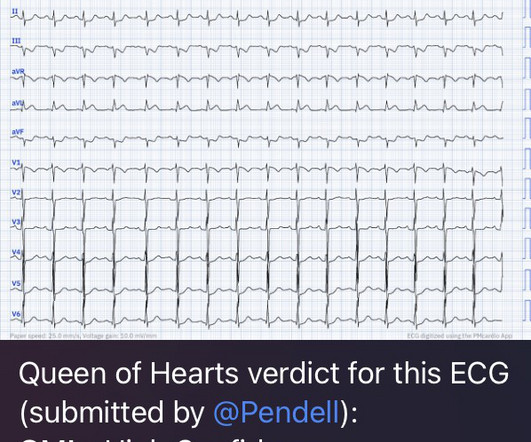
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chest pain. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. Keep an eye on the blog as an OMI QUIZ soon will be published where you test yourself vs the Queen!
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System.
No known risk factors for ACS/CAD. A medic sent this case A 33 yom who presented to an urgent care facility with a complaint of chest pain for several days. His chest pain started after he began taking a testosterone supplement.
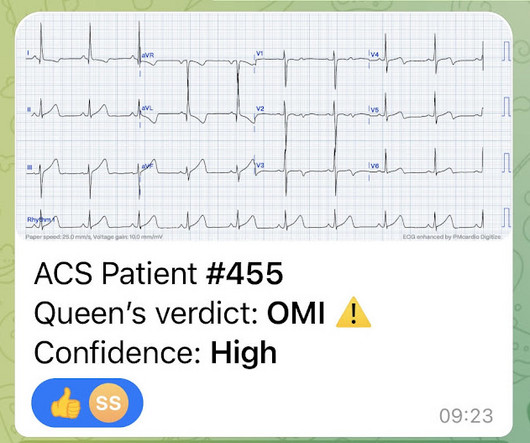
This is for the version housed on Telegram: [link] You can get the full PM Cardio app here if you live in the UK or EU (or say you do upon registration): [link] Case Continued The cath lab was activated and the patient received 180 mg of ticagrelor, and then was transported to the cath lab.
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. 1] European guidelines add "regardless of biomarkers".
With API , participating CAD and RMS vendors will be able to automatically send data back and forth to NERIS. For any CAD and RMS vendors who are interested, you can share information and ask questions during the USFA development tea m’s regular NERIS office hours.
PEARL #2: = Aslanger's Pattern: Examples of Aslanger's Pattern appear in a number of cases in Dr. Smith's ECG Blog ( This pattern is very nicely described by Dr. Smith in the January 4, 2021 post). Patient stated that he has had glucose over 400 even though he has not missed any doses of insulin.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. This is a re-post of an excellent case from 2021. See it again now, along with our new Queen of Hearts functionality. We've come a long way in 2 years! And the pace only quickens.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
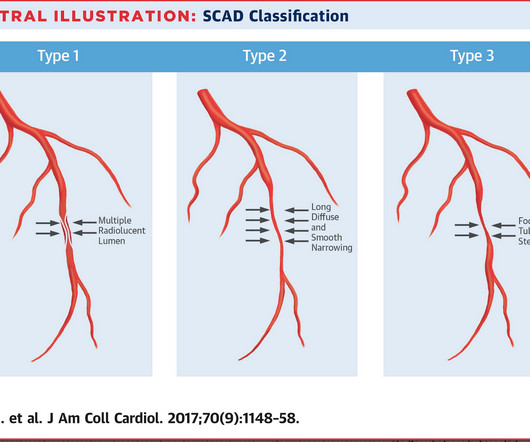
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. This case occurred 10+ years ago.
The ED provider ordered a coronary CT scan to assess the patient for CAD. Regular readers of Dr. Smith's ECG Blog are well familiar with what is perhaps my favorite Stephen Smith Adage = "You diagnose acute pericarditis at your peril!" Another blood pressure was checked.
Transferred to our ED and taken to cath lab Cath- mild nonobstructive CAD, mild mid LAD bridge Echo- EF 65-70%, normal wall motion, no diastolic dysfunction. "Feels like a fake to me, but would be an awful miss so I would be very careful 4. STE from lead I all the way around to lead III would be pretty unusual for OMI, I guess."
He had no previous history of CAD, and presented with very typical waxing and waning chest pain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. I saw this 59 year old male 3 weeks ago. Blood pressure was 150/80.
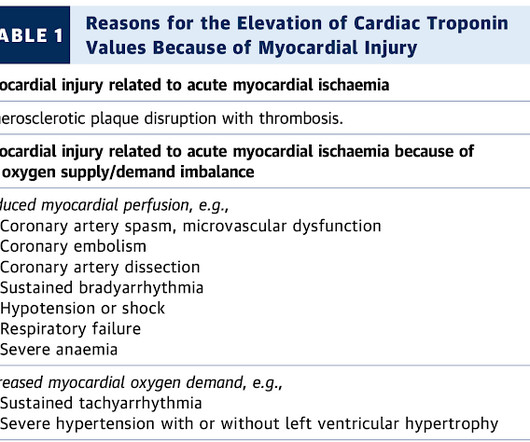
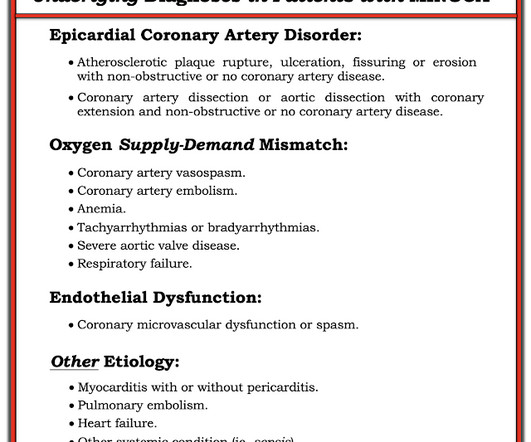
Diagnosis of MINOCA should be made according to the Fourth Universal Definition of MI, in the absence of obstructive coronary artery disease (CAD) (no lesion ≥50%). The authors recommend using optical coherence tomography or intravascular ultrasound imaging in patients with evidence of nonobstructive CAD by angiogram. myocarditis).
This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB. There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL).
He had a history of CAD with CABG. A middle-aged male had a V Fib arrest. He had not complained of any premonitory symptoms (which is very common). Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. There is profound ST depression especially in I, II, V2-V6.
So, I'm a follower of your blog, and I think I have a interesting case that I attended yesterday." Angiogram soon after (around 4 hrs after presentation) showed multi vessel CAD, with culprit lesion total occlusion of the first obtuse marginal branch (OM1), which was stented. Risk Factors: High Cholesterol. Vitals Signs: Normal."
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc.
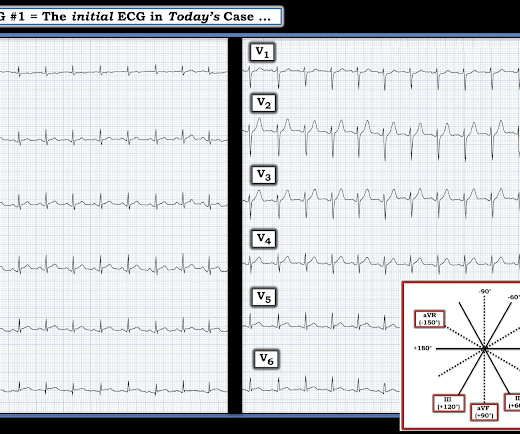
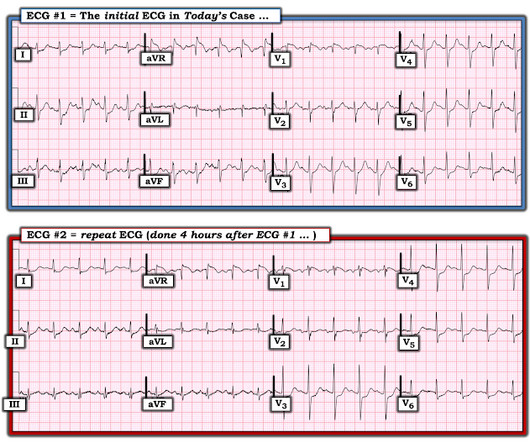
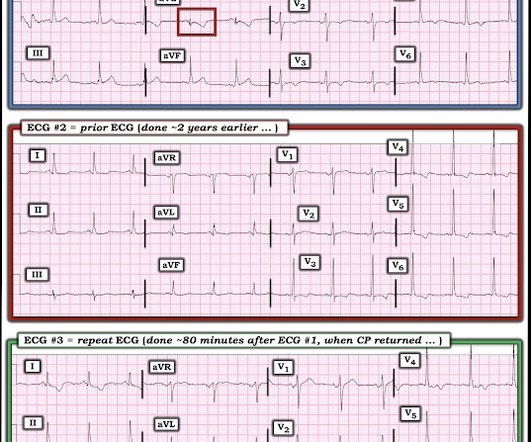
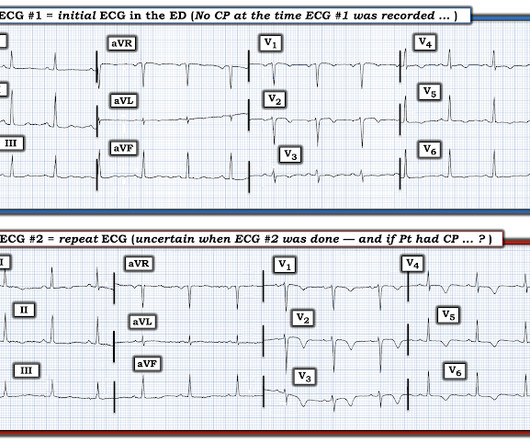
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted.
Inferior STEMI s/p DES with significant residual LM/left sided obstructive CAD : TnI 11,344 on admission, suggesting significant infarct prior to presentation. Subsequently, determined that the patient was too unstable for transfer in the current state. Hence, decision made to ECMO cannulation prior to transfer.
On May 6, 2024, version 1 of NERIS core data schema was released, including: Fire Department (Entity) Specification CAD/Dispatch schema Incident schema Since the upgrade was announced, ESO’s Fire Incidents team has been preparing and planning to ensure your team will be ready for the transition to NERIS.
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. I could have told you this (and did tell you this) without an MRI.
He had a family history of early CAD and occasional drug and tobacco use. It is not yet available, but this is your way to get on the list. link] Here is the history: A 30 yo man presented complaining of severe chest pain. The ECG was alarming to the ED physician who did indeed review it.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. In Figure-1 I have excerpted from the above blog post, the Pearls of Wisdom from Drs.
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. As we have described multiple times on this blog, false positive "pericarditis" kills by distracting the clinician from actual emergencies including OMI, dissection, PE, and others. A repeat ECG was performed and cardiology was re-consulted: Roughly unchanged.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. There was no prodrome and no associated symptoms such as SOB or CP. The medics recorded an ECG: There is STE in V1-V3 and aVL, with reciprocal ST depression in II, III, aVF. The medics were worried about STEMI, as it meets STEMI criteria. What do you think?
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? He also had non-acute CAD of the RCA (50%) and LCX (50%).
CAD-RADS category 1. --No For interested readers, in My Comment in the August 12, 2022 post of Dr. Smith's ECG Blog — I reviewed the original 1982 description of this Syndrome by de Zwaan, Bär & Wellens — and correlated this original description with our understanding of this Syndrome today. A CT Coronary angiogram was ordered.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
He has a history of known CAD, diabetes, and dyslipidemia. This post was written by one of our fantastic Hennepin County Medical Center Emergency Medicine interns who is an ECG whiz, Daniel Lee. A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content