This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
What They Did: Investigators performed a retrospective cohort study in the EmergencyDepartment at the University of Michigan between July 1, 2014 through December 31, 2018. Comorbidity Index : Higher in the cefepime group (median 2 vs. 1). 9 Instrumental Variable Analysis? vs. 52.2%). vs. 15.3%). vs. 22.3%).
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. g/dL, thrombocytopenia of 96 10 9 /L, prothrombin time (PT) of 16.1 1 By the end of 2023, 117.3 million people had been forcibly displaced, representing 1 in 69 individuals or 1.5% seconds (normal 30-40 seconds), creatinine of 3.11
2024 Oct 9. You can find more details in the full blog post. There were no differences in survival (12% with IO vs 10% with IV) or neurologically intact survival (9% vs 8%). Acad Emerg Med. 2024 Nov 1. doi: 10.1001/jama.2024.20424. 2024.20424. Which is better in out of hospital cardiac arrest: IV or IO?
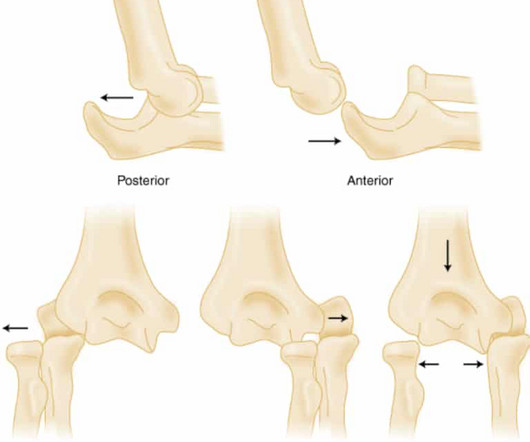
About 1 in 10 patients will have an occult fracture, and roughly 1 in 10 scaphoid fractures result in nonunion. 1,2 However, the risk of nonunion among patients with MRI-confirmed occult fractures is much lower—around 1 in 30. 2025;26(1):14. 7 🧾 Paper Cohen A, Reijman M, Kraan GA, et al. J Orthop Traumatol.
1 They noticed how spontaneously breathing patients had their IVC collapse with inspiration; and ventilated patients had their IVC dilate during positive pressure ventilation. RESUS SCENARIO Picture this: you just arrived at your shift at the local emergencydepartment. Oct 2013; PMID: 24079262 Gohar E, et al.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think?
In many emergencydepartments (ED), US machines are readily available and can be used to rapidly assess and monitor patients with acute dyspnea at the bedside. What They Did: Design: Randomized, controlled, blinded-outcome trial Sites: Three emergencydepartments in Denmark Duration: October 9, 2019 to May 26, 2021.
patients that take ACE inhibitors (but 20-30% of all angioedema presentations to the EmergencyDepartment) 3 times more common in Black Americans ( Kostis 2005 ) 0.01 patients that take ACE inhibitors (but 20-30% of all angioedema presentations to the EmergencyDepartment) 3 times more common in Black Americans ( Kostis 2005 ) 0.01
Epidemiology 1 to 2.4 cases per 100,000 people ( Zimmerli 2010 ) More common in males with M:F of 3:1 Rate is also increasing due to increased number of spinal procedures Typically affects adults, with most cases occurring in patients over 50 years old. Other pathogens include: E. Orthopedic Emergencies 2015 May; 33(2) 311-26.
Spikes 2, 3, 4, 5, 7, 8, and 9 all occur either during or immediately after P waves which should never happen. Repeat ECG from the emergencydepartment is shown. Regarding Today's Tracing: For clarity in Figure-1 — I have reproduced and labeled the initial ECG in today's case. The radiologist did not comment on this.
This blog is an example of exactly that. While transporting to the emergencydepartment, the patient’s mother informed me that PDCD affects less than 1 in 50,000 individuals and is more common in males than females. 2007 9. van Dongen S, Brown RM, Brown GK, Thorburn DR, Boneh A. Never stop looking for it.
Impact of intravenous calcium with diltiazem for atrial fibrillation/flutter in the emergencydepartment. Am J Emerg Med. What They Did: Researchers conducted a multicenter, retrospective cohort study in three community hospitals and two freestanding emergencydepartments. Article: Rossi N et al.
Sites: Investigators recruited patients at 31 French emergencydepartments at university and nonuniversity hospitals Duration : June 1, 2009 to March 31, 2015. Recurrence of pneumothorax within 1 year. Pneumothorax recurrence within 1 year: 20% for aspirations, 27% for chest tubes. Panacek, E. Strange, C.,
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion.
CT head without contrast 1 is performed and reveals the following: Question: What is the diagnosis? Updated November 9, 2023. Clinical Policy: Use of Intravenous Tissue Plasminogen Activator for the Management of Acute Ischemic Stroke in the EmergencyDepartment. Ann Emerg Med. Erratum in: Ann Emerg Med.
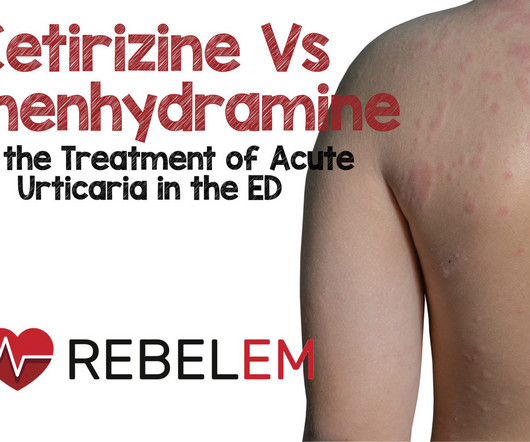
Patients were randomized in a 1:1 ratio. Risk of first-generation H(1)-antihistamines: a GA(2)LEN position paper. Multicenter study of emergencydepartment visits for insect sting allergies. 2005 Sep;116(3):643-9. Multicenter study of emergencydepartment visits for food allergies. 2, 2001, pp.
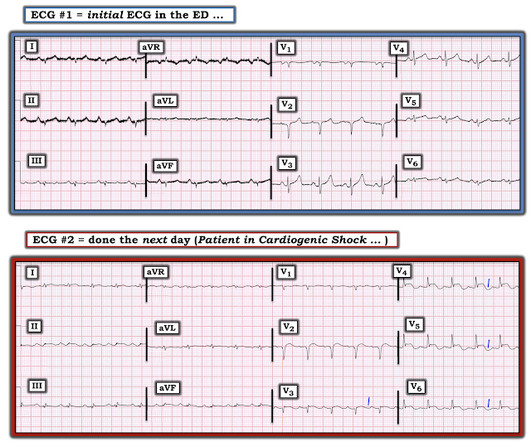
The patient’s ECG on arrival at the emergencydepartment is shown below. For clarity — I’ve put these 2 tracings together in Figure-1. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3). No arrhythmias occurred en route.
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. JAMA Intern Med 2019 9. Am J Med [Internet] 2017;130(9):1076–83.e1.
Read More REBEL EM: The Ketorolac Analgesic Ceiling References Irizarry E et al. Acad Emerg Med 2021; 28(11): 1228-35. Can J Emerg Med 2007; 9(1): 30-2. NSAID use and efficacy in the emergencydepartment: single doses of oral ibuprofen versus intramuscular ketorolac. Ann Emerg Med 1995;26:117-20.
PSA, also referred to as intravenous sedation in this paper, requires considerable resources, including 1:1 nursing observation, and burdens the emergencydepartment (ED). weight of the entire meta-analysis, and 9/12 carried more than 8% weight. J Emerg Med. 1995 Jan-Feb;13(1):37-42. PMID: 7782623.
Read More REBEL EM: The Ketorolac Analgesic Ceiling References Irizarry E et al. Acad Emerg Med 2021; 28(11): 1228-35. Can J Emerg Med 2007; 9(1): 30-2. NSAID use and efficacy in the emergencydepartment: single doses of oral ibuprofen versus intramuscular ketorolac. Ann Emerg Med 1995;26:117-20.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. Pol Arch Intern Med. 2017;127:401–411.
Am J Emerg Med. 2013 Sep;31(9):1389-92. The NoPAC trial, which was published in 2021,(1) compared TXA to placebo in a large multicenter randomized control trial in the UK which looked at data from 26 emergencydepartments. Ann Emerg Med. PMID: 33612282 Janapala RN, Tran QK, Patel J, Mehta E, Pourmand A.
Here is the parasternal short axis, performed by a real expert in emergencydepartment point of care cardiac ultrasound: There does not appear to be an anterior wall motion abnormality. I was relieved to see this MRI result: MRI IMPRESSION 1) Mildly decreased LV function with no focal wall motion abnormalities. Pericarditis?
Background: The use of ultrasound is well established for trauma patients in the emergencydepartment, with almost every patient receiving a FAST (Focused Assessment with Sonography in Trauma) examination as part of the “ABC’s” of trauma. 2022 Jan 1;92(1):44-48. 2015 Jan;39(1):172-8. Acad Emerg Med.
Written by Destiny Folk MD, with edits by Meyers, peer reviewed by Smith and Grauer A woman in her late 20s with a past medical history of cervical cancer status post chemotherapy and radiation therapy presented to the emergencydepartment for shortness of breath, chest tightness, and two episodes of syncope. 2013 Sep;26(9):965-1012.e15.
A Deep Neural Network learning algorithm outperforms a conventional algorithm for emergencydepartment electrocardiogram interpretation. S-wave is in V2 = 17 mm S-wave V4 = 9 mm Total = 26 (not greater than 28), so not LVH by the new rule! For clarity — I’ve reproduced this ECG, to which I’ve made a few additions ( Figure-1 ).
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
You are the Paediatric doctor on call and receive a call for an incoming patient to the emergencydepartment. Tragically, several attempts at resuscitation upon arrival at the emergencydepartment were unsuccessful. Intensive Care Research , 1 (3-4), pp.60-64. This blog, like the paper cited, is dedicated to him.
emergencies, patient’s request). However, actual increases in available services in emergencydepartments based on prior state-level requirements have been mixed. K-International/TheLanguage Blog website. Department of Health and Human Services website. 2022;105(1):62-73. Regenstein M, Anders E, Wynia MK.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. Stein et al.
1 His description of cases of life-threatening infections in the perineal, genital or perianal regions were thought to be idiopathic in previously healthy men. 3-5 Fournier gangrene is a type of necrotizing soft tissue infection, which can be categorized into four types based on the infectious organism involved and other features (Table 1).
Comparison of the MASCC and CISNE scores for identifying low-risk neutropenic fever patients: analysis of data from three emergencydepartments of cancer centers in three continents. 2011 Jun;153(6):773-9. Ann Emerg Med. Neutropenic Fever: Fever (one reading of 38.3C Support Care Cancer. 2018 May;26(5):1465-1470.
Here they are: Learning Points: 1. Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in EmergencyDepartment COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. Am J Med [Internet] 2017;130(12):1431–9.e4. Clin Chem [Internet] 2017;63(1):101–7.
titled "The Association of Rocuronium Dosing and First-Attempt Intubation Success in Adult EmergencyDepartment Patients" revealed that first-attempt intubation success was the highest when more than 1.4 mg/kg Rocuronium versus 1 to 1.5 mg/kg Rocuronium versus 1 to 1.5 mg/kg of Rocuronium was used [4].
Previously, I wrote a blog on pre-oxygenation, referencing my personal “weapon of choice” as chosen from the 7 Ps of RSI. But, putting them both into one blog would make for a read far too long to maintain even my attention span (which honestly is pretty short). Why is Physiologic Optimization Important?
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. J Am Coll Cardiol 53(17):1503-9. Plum mer D, Dick C, Ruiz E, Clinton J, Brunette D. Emergencydepartment two-dimensional echocardiography in the diagnosis of nontraumatic cardiac rupture. Ann Emerg Med 1994;23(6):1333-42.
Over 1,500 children in EDs, aged 1 to 4 with acute hypoxemic respiratory failure needing hospital admission, across 14 emergencydepartments in Australia and New Zealand were randomly allocated 1:1 to high-flow oxygen therapy OR standard oxygen therapy (approximately 750 children in each group). days compared to 1.50
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. He found 2 ECG patterns of atypical T-wave development in PIRP: 1) persistently positive (upright) T-waves 48 hours after AMI onset. Lessons : 1. Although rupture has a high mortality, it is not uniformly fatal References 1.
1 That is the last line in Dr. Robert Ray, Jr.’s s eye-opening and intensely raw blog, where he details his experiences with institutional and systemic racism during his emergency medicine residency. 2006;98(9):1415-24. “I matter, now what are you gonna do?” We may think that there is nothing wrong with those responses.
One of the most hair-raising presentations to the emergencydepartment (ED) can be massive hemoptysis with respiratory failure. or 9 size endotracheal tube to allow for bronchoscopy and/or endobronchial blocker placement whenever necessary. He is the founder and host of Emergency Medicine Cases podcast and website.
1-6 We now have the Community-Acquired Pneumonia: Evaluation of Corticosteroids (CAPE COD) Trial. Patients admitted to the ICU with severe community-acquired pneumonia were randomized in a 1:1 ratio to receive hydrocortisone or a placebo. However, except for one trial, none showed a between-group difference regarding mortality.
This blog post aims to help familiarise you with some of the most common reasons for prescribing antibiotics in the paediatric emergencydepartment. Antibiotic Use for Common Infections in Pediatric EmergencyDepartments: A Narrative Review. Addo-Yobo E, Chisaka N, Hassan M, Hibberd P, Lozano JM, Jeena P, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content