This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
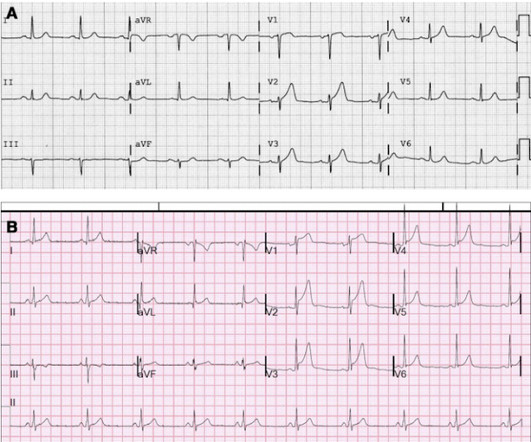
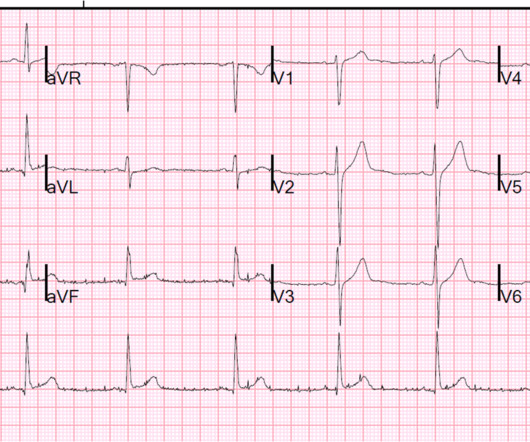
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria. Figure-1: ECG from the August 26, 2009 post in Dr. Smith's ECG Blog.
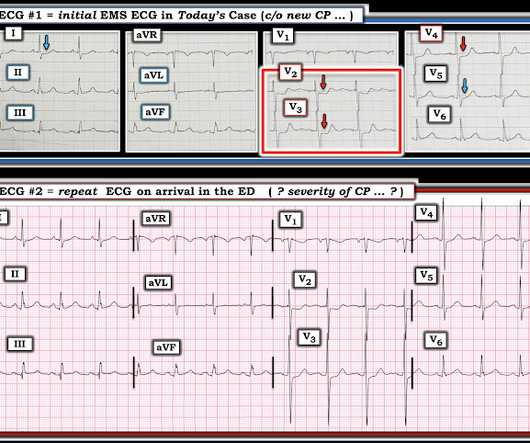
Here is the prehospital ECG: The computer says STEMI Based on this and the presence of chest pain, the medics did a prehospital activation of the cath lab. A 40-something male complained of 3 days of chest pressure. He called 911. He had some pulmonary edema and hypoxia. What do you think? Interpretation: There is clear atrial flutter.
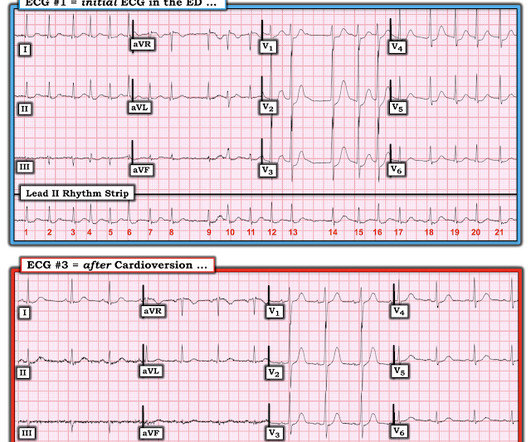
interesting spontaneous reperfusion case 1413140 prehospital STEMI first ED ECG is here, with 3/10 pain: But this is the same patient just 10 minutes before, with 7/10 pain Isn't it ridiculous to say that the patient has both a STEMI and an NSTEMI? ACS is dynamic. It can't be given one static name. Now the patient has one disease: OMI.
The subsequent diagnosis of an ST-segment elevation myocardial infarction (STEMI) sets forth a cascade of events that typically culminates in the patient being transported to hospital capable of emergent percutaneous coronary intervention (PCI). However, the notion of “STEMI equivalents” has gained traction.
Diagnosis: Atrial Fibrillation with complete (3rd degree) AV block and inferoposterior STEMI. In the 1980's, it was believed that the right precordial ST depression that frequently accompanies inferior STEMI was due to "anterior subendocardial ischemia." Heart block in inferior STEMI is due to ischemia of the AV node.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. 2020) If you are a regular reader of this blog this diagnosis will be easy for you, and you will manage this type of patient correctly with immediate revascularization.
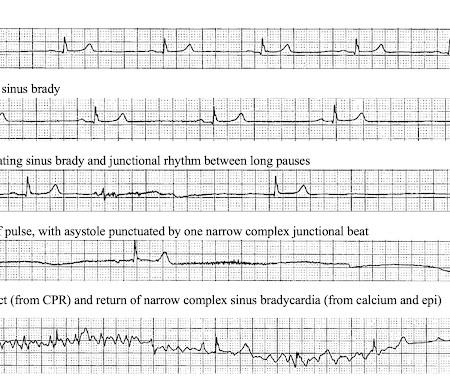
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. Later in the night, the patient became bradycardic and developed a Mobitz II pattern , but he remained asymptomatic and hemodynamically stable.
On your blog I appreciate the QOH ECGs that highlight where the QOH is looking. Serial ECG's obtained, none meeting true STEMI criteria, but dynamic changes noted. The STEMI alert to OR prep time for CABG was around 60 minutes and this exemplifies excellent, expedient teamwork. We are hopeful for her recovery.
But if there’s natural ST segment elevation and depressions all over a left bundle branch block, how do we know when a patient is having a STEMI or not? V5 follows the Law of Appropriate Discordance. Enter the Sgarbossa Criteria.
Case continued: A STEMI alert was paged out, the cath lab was activated, and the cardiologist was sent the ECG. His reasoning was that the EKG I sent him was consistent with Brugada and not a STEMI. We gave 4000U heparin, ASA, and sublingual nitro taking his pain from a 9 to a 2. ng/mL) The repeat troponin 6 hours later was 4.5,
It is tempting to say that the ST depression was "posterior STEMI" on these initial ECGs, but that is not so. The ST depression was not V1-V3 (as in posterior STEMI), but rather V3-V6 (which is what is seen in subendocardial ischemia). Comment 2: This is a great example of how the dichotomy between STEMI and Non-STEMI is false.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. Inferior STEMI with AV Block, Cardiogenic Shock an.
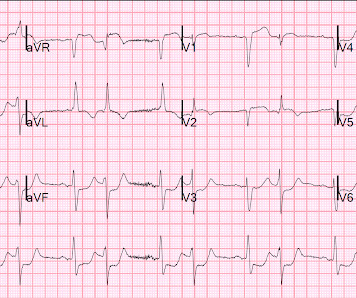
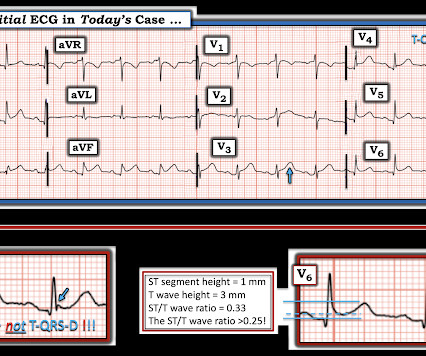
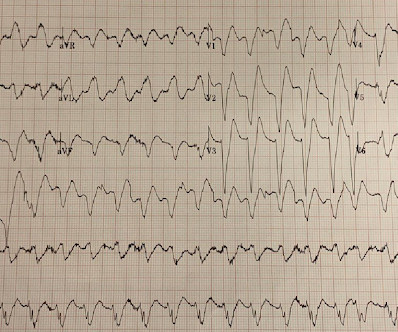
The Zoll algorithm impressively stated: STEMI A paramedic student had the PMCardio AI Queen of Hearts on his phone and this is what it reported: New PMcardio for Individuals App 3.0 There is a hyperacute T-wave in V6, which is the lateral part of the posterior wall and a common supportive finding in posterior OMI.
There is ST Elevation in V1-V3, but clearly not due to STEMI. He was sure the doctors did not tell him that his brother succumbed to occlusion in the coronary arteries. Here is his ED ECG: Day 1, "Hampir Stroke," temp 39 degrees : What do you see? This is Classic Type I Brugada Morphology.
Thus, the ACC/AHA 2013 STEMI guidelines now list diffuse ST depression, with ST elevation in aVR, as an indication for thrombolytic therapy. I discuss this more at this post: ST Elevation in Lead aVR, with diffuse ST depression, does not represent left main occlusion.
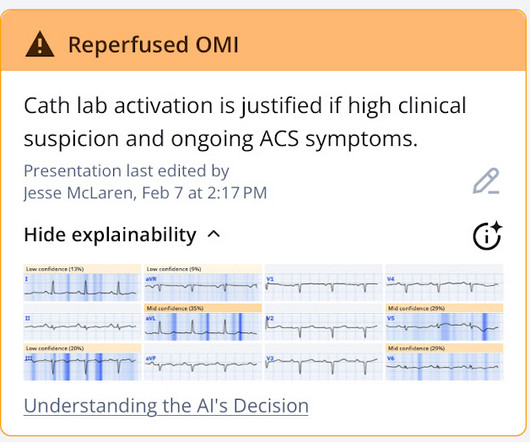
The PMCardio Queen of Hearts app asks you, before giving an interpretation of OMI ("STEMI-Equivalent"), whether the patient's clinical presentation is high risk for OMI. Dizziness is so unlikely to be OMI without an obvious ECG, that I am going to pretend that this patient presented with chest pain. So let's pretend this is acute chest pain.
You probably know that the risk of LV free wall rupture is high if thrombolytics are given >14 hours after symptom onset - [link] gov/pubmed/2142705 ; this is also referred in STEMI guidelines. So it may be reasonable to mention that cautionary point.
A prehospital ECG showed ST Depression in V1-V3 and the medics were concerned for posterior STEMI. Charts showed a history of some mitral regurgitation and an enlarge left atrium, as well as hypertension treated with a thiazide diuretic. Pulse was 128 and irregular, BP was 141/75.
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI. Mostly the same findings and reasoning as the current ECG.
Now as an intern, he is exceptional at EKG interpretation because he was able to learn of the OMI paradigm and importance of pattern recognition before getting poisoned by years of learning STEMI. This is really a transient OMI (or transient STEMI if one uses that terminology and it has diagnostic ST Elevation).
The differential is: 1) LAD occlusion proximal to the septal perforator with wraparound to inferior wall (that much STE in V1 is quite specific for septal involvement with anterior STEMI) vs. 2) Proximal RCA with RV involvement. Is it important to know whether this is LAD or RCA? Somewhat, but not hugely important.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
This is almost certainly an acute inferior MI, though does not meet mm "criteria" for STEMI --The beginnings of T-wave inversion suggest an open artery. Because this "anterior" MI is due to STEMI of the right ventricle (RV) , not of the LV. ng/mL due to the brief RV STEMI. It may be due to RV STEMI, which is also anterior.
This was interpreted as "inferior STEMI" and the cath lab was activated. Discharge diagnosis was Non-STEMI. The STEMI/NSTEMI dichotomy can make it difficult to identify the culprit lesion, which can be spontaneously reperfused at the time of the angiogram 3. The patient had no further episodes of chest pain.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! As I emphasized in My Comment in the February 27, 2023 post in Dr. Smith's ECG Blog some patients may develop everything except QRS widening. HyperKalemia with Cardiac Arrest.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. Is this inferor STEMI? LV Aneurysm?
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. inferior MI, first 2 EKGs missed, EKGs in umn emai.
Importantly, one trial of 925 consecutive STEMI-positive occlusion myocardial infarctions found that 26% had presentation troponin values < 99th percentile when then presented less than 2 hours from symptom onset and 14% had values < 99th percentile when they presented with symptoms for greater than 2 hours.
This ECG was recorded 30 minutes later with ongoing pain: Queen of Hearts says no signs of STEMI or Equivalent for both: New PMcardio for Individuals App 3.0 Midwest STEMI Consortium: decreased false positives by 33% (presented at ACC Quality Summit San Antonio 2024) 3. She denied preceding symptoms or recent illnesses.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. LBBB and Respiratory Failure Subacute STEMI.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. The delay between OMI and STEMI claims yet another.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. Updated 1 hour lecture: The False STEMI-NonSTEMI D.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. A Patient with Cocaine Chest Pain and Prehospital.
OMI Manifesto About Resources Teaching Images Lectures + Podcasts Rules + Equations OMI Literature Timeline OMI Facts and References The OMI Quizzes OMI Pocket Guide Cardiac CATH Guide QTc Calculator Lead Reversals-Artifact Neuroprotective CPR OMI AI: The Queen of Hearts Sunday, August 25, 2013 Anterior ST Elevation - Is it STEMI?
How well does the computer interpretation perform? -- in this case, the computer diagnosed STEMI but the patient had Fever with Brugada -- A young F is hyperthermic, delirious, and dry: Fever-induced Brugada? Syncope and ST Segment Elevation. And another finding. Diphenhydramine toxicity?
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. anterior STEMI, VT, head bleed from stab conf, Cou.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents. From Scott Weingart EMCrit Interview: Who needs th.
Translate Follow us on X (Twitter) Follow @smithECGBlog Follow @PendellM Follow @ekgpress Follow @AslangerE Follow @ecgcases Follow @PMcardioBot Total Pageviews Use this Blog as a Textbook I highly recommend using this blog as an atlas or textbook. Some are STEMI-equivalents.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content