This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
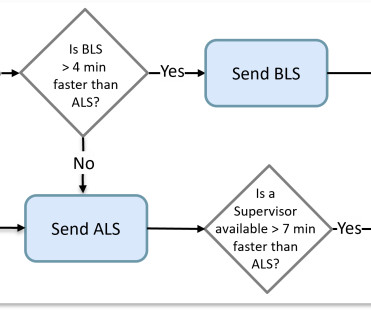
Some computer-aided dispatch (CAD) software did better than others by considering the average travel time of an actual route instead of allowing nearness to be determined by a straight-line distance. It was a matter of determining which crew was available closest to the scene.
Connections with CAD, Billing, and Patient Outcomes Seeing the full picture of a patient’s care is key, and new technology is making the response for prehospital care faster and more efficient than ever.
2. Coronary angiography reveals significant and severe CAD involving all three epicardial vessels. Abnormal gated wall motion of the LV with an ejection fraction of 18%. He was taken to the Cath Lab. RCA Left Main / LAD / LCX Cath dictation 1. Moderate sedation.
He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. For this box, please keep ventricular tachycardia (VTach) and supraventricular tachycardia with aberrancy (SVT with aberrancy) in your differential. This EKG comes from a 75-year-old male presenting with palpitations. Take a look: Figure 3. Did you read it?
He denied any known history of CAD, but did report ASCVD risk factors to include HTN, HLD, and DM. David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
Patient 2 A man in his 50s with history of CAD and prior PCI, diabetes, presented with acute constant chest pain for the past few hours. Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. He was discharged home.
Were making the jump to general availability (GA) and adding new features such as CAD and Cardiac Monitor integrations, Longitudinal Record (LR), and Mobile-to-Mobile functionality. This basic version will not include auto-import configuration, and integrations with CAD and EHR will not be added until upcoming releases in 2025.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. Edited by Smith He also sent me this great case.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System.
Because if such severe CAD is present, the patient is likely to need CABG. They show that if there is not >/= 1 mm STE in aVR, then ACS is highly unlikely to be due to severe 3-Vessel disease or Left Main. why is this important? If they need CABG, then the surgeon will usually be unhappy if the patient received clopidogrel.
consult: In summary, this is a 47 year old male with past medical history of CAD s/p STEMI in 2010 s/p PCI to LAD with BMS, HTN, tobacco, alcohol and substance abuse that presented with chest pain and found to have ST elevation with T wave inversion in his ECG. Patient had blood cultures drawn.
Metoprolol Considerations: Dosing (5 mg every 10-15 minutes, max 15 mg), benefits in CAD and HF, limitations in asthma/COPD patients. Treatment Approaches for AF Types General Rapid AF: First Line Agents: Metoprolol vs. Diltiazem. Diltiazem Advantages: Faster action, suitability in asthma/COPD, typical dosing (0.25 mg/kg if needed).
A patient with history of severe CAD, CABG, with all native vessels occluded, on maximal medical therapy presented with his typical angina. NSTEMI: Patient with known severe CAD presenting with troponin elevation up to 21 and chest pain that was refractory to initial nitroglycerin therapy suggestive of unstable angina.
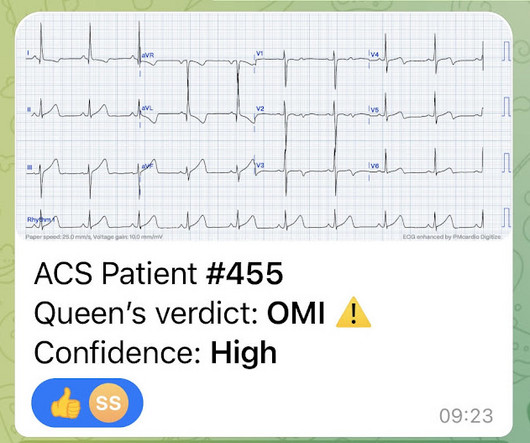
This is for the version housed on Telegram: [link] You can get the full PM Cardio app here if you live in the UK or EU (or say you do upon registration): [link] Case Continued The cath lab was activated and the patient received 180 mg of ticagrelor, and then was transported to the cath lab.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chest pain. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. How would you assess this ECG? How confident are you in your assessment? What is your next step?
In 2002, Jennifer transitioned to the Broomfield Police Department in Colorado where she dispatched and served as an Emergency Medical Coordinator, Communications Training Officer, Public Education Coordinator, and Computer-Aided Dispatch (CAD) Project Lead.
With API , participating CAD and RMS vendors will be able to automatically send data back and forth to NERIS. For any CAD and RMS vendors who are interested, you can share information and ask questions during the USFA development tea m’s regular NERIS office hours.
Once the new system is in place, it will also be able to integrate information from the computer-aided dispatch system (CADS). Implementation and Benefits NERIS will require a significant update to the current records management system software, or alternatively, the use of a new free app for collecting incident data.
With FirstWatch, I get alerted through CAD triggers on my phone as soon as that call comes through. Having instant access to CAD data allows me to do this.” Lay of the Land It’s not just the CAD data the chief appreciates. “I PD continues to innovate, despite staffing challenges Chief Jeffrey Beazizo of the Lake Stevens, Wash.,
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. This is a re-post of an excellent case from 2021. See it again now, along with our new Queen of Hearts functionality. We've come a long way in 2 years! And the pace only quickens.
We hope to have a basic NERIS-compliant beta early in 2025, with additional updates (CAD imports, ESO EHR integration, ESO Insights reporting, etc.) It will be a simplified version and may not yet be ideal for agencies with ESO suite integrations like CAD and EHR imports. The timeline may vary.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. CASE 1 A 45 y/o Male called 911 for new onset central chest discomfort, non-radiating, 5/10 pain scale, and without any vomiting, diaphoresis, or pallor. A 12 Lead ECG was recorded.
Your existing historical CAD records contain the necessary information to build such dynamic views in real-time. The existence of identifiable causes explains the ability to properly forecast the vicinity of calls in addition to their timing.
This included date, POE, patient demographics, chief complaint, computer-aided dispatch (CAD), provider impression (diagnosis), and time out of service. The El Paso Fire Department (EPFD) provided data for all encounters between February 2017 and January 2023.
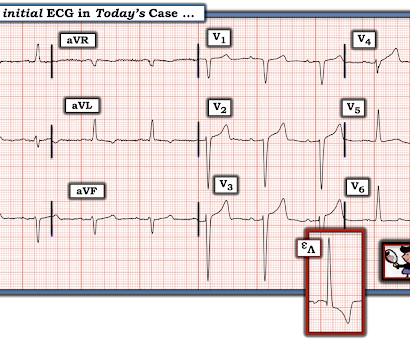
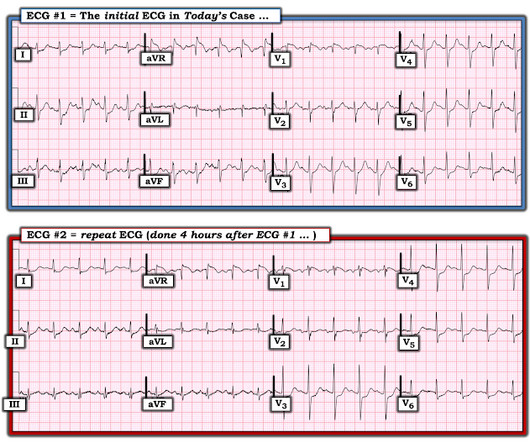
These concerns were readily conveyed to my supervising cardiologist with particular emphasis on high pretest probability for baseline advanced CAD (3-vessel disease, specifically) with a critically stenosed proximal LAD. A quick way to validate this conjecture is to simply acquire a secondary ECG, but I failed to do this in the moment.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
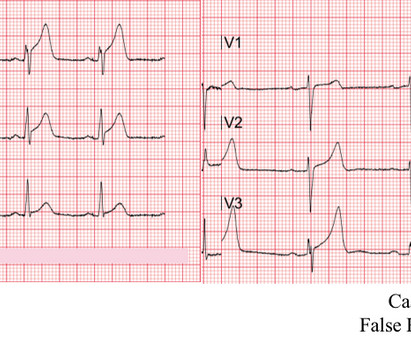
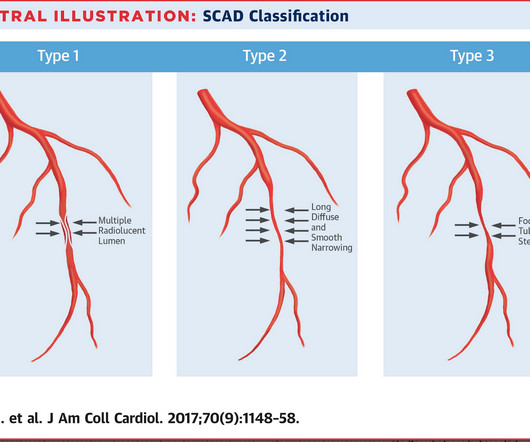
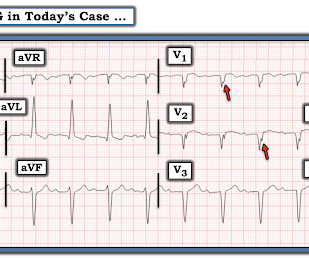
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. This case occurred 10+ years ago. Excellent description by Dr.
Transferred to our ED and taken to cath lab Cath- mild nonobstructive CAD, mild mid LAD bridge Echo- EF 65-70%, normal wall motion, no diastolic dysfunction. "Feels like a fake to me, but would be an awful miss so I would be very careful 4. STE from lead I all the way around to lead III would be pretty unusual for OMI, I guess."
Angiogram The patient did go for an angiogram and there was no occlusion present, and no definite culprit, although there was diffuse CAD and one possible culprit: "There is a medium-large caliber OM3 with 40-50% stenosis in the mid-segment and lumen irregularity that could suggest dissection or plaque rupture, but TIMI III flow throughout."
He had no previous history of CAD, and presented with very typical waxing and waning chest pain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. I saw this 59 year old male 3 weeks ago. Blood pressure was 150/80.
This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB. There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL).
He had a history of CAD with CABG. A middle-aged male had a V Fib arrest. He had not complained of any premonitory symptoms (which is very common). Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. There is profound ST depression especially in I, II, V2-V6.
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. 1] European guidelines add "regardless of biomarkers".
There are five NERIS Fire Data Standards currently in development today – they are: core fire data specification, CAD interface standard and API guide, incident, investigative, and exposure data standards. What are the milestones? NFIRS will remain operational throughout the completion and launch of the new NERIS system.
Multivessel CAD 2. The calculated post stress ejection fraction is 44%. Inferolateral/anterolateral/inferior akinesis noted. EKG reveals marked ST segment depression at rest and following stress. Cardiology consult impression 1. Ischemic cardiomyopathy, EF 45 --> 20% 3.
Diagnosis of MINOCA should be made according to the Fourth Universal Definition of MI, in the absence of obstructive coronary artery disease (CAD) (no lesion ≥50%). The authors recommend using optical coherence tomography or intravascular ultrasound imaging in patients with evidence of nonobstructive CAD by angiogram. myocarditis).
No known risk factors for ACS/CAD. A medic sent this case A 33 yom who presented to an urgent care facility with a complaint of chest pain for several days. His chest pain started after he began taking a testosterone supplement.
As the pregnant population continues to age and with RF and smoking and DM still common we can expect to see pregnant woman with CAD. Well, most commonly we’re going to see ACS. Pregnancy itself with its bump in plasma volume, reduced Hb and increased cardiac output is like one long exercise stress test.
Inferior STEMI s/p DES with significant residual LM/left sided obstructive CAD : TnI 11,344 on admission, suggesting significant infarct prior to presentation. Subsequently, determined that the patient was too unstable for transfer in the current state. Hence, decision made to ECMO cannulation prior to transfer.
Increased risk in those with preexisting CKD, other risk factors for renal disease (HTN or CAD), and those on ACEIs/ARBs. AKI associated with GLP-1 agonist therapy is prerenal in nature and associated with nausea, vomiting, diarrhea, and reduced oral intake.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content