This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For instance, there was no protocol for stroke or STEMI. I dont the exact year these protocols were implemented, but I know that in 2008 they went from a simple typed document to an algorithm format. The document was 222 pages, including 42 medications, 14 procedures, as well as 14 policies.
In addition to standard patient demographics (mean age of 81), the authors looked for complete sets of vital signs (85%), abnormal vital signs and ambulation assessment documentation (42%) during the patient’s first encounter. It is also important to determine and document the patient’s capacity to refuse transport.
It is essential to ensure that cost reports are meticulously documented, auditable, and aligned with allowable cost definitions under federal law. Cost shifting has been well-documented in health policy literature and poses a significant threat to the sustainability of both EMS systems and broader healthcare markets.
All services provided can be documented and billed, reducing missed revenue. Existing clinical dashboards include specific measures for stroke and STEMI. With the ESO HDE EMPI match: All responding agencies receive patient outcome information.
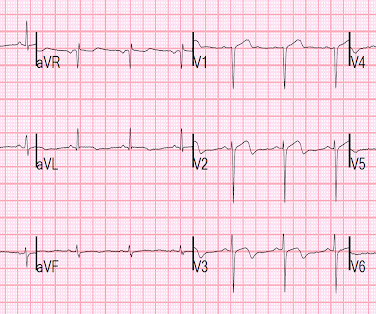
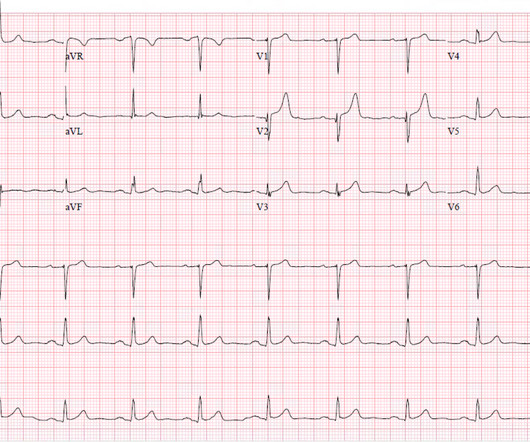
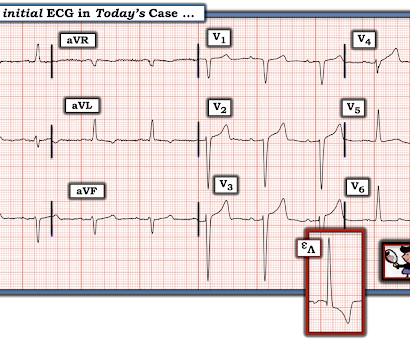
There is ST Elevation in V1-V3, but clearly not due to STEMI. What makes this particularly interesting is the documentation of the change in morphology as the fever resolves. He was sure the doctors did not tell him that his brother succumbed to occlusion in the coronary arteries. This is Classic Type I Brugada Morphology.
Now as an intern, he is exceptional at EKG interpretation because he was able to learn of the OMI paradigm and importance of pattern recognition before getting poisoned by years of learning STEMI. This is really a transient OMI (or transient STEMI if one uses that terminology and it has diagnostic ST Elevation).
Unexplained cardiac arrest or documented VF/polymorphic VT: +3 3. How well does the computer interpretation perform? -- in this case, the computer diagnosed STEMI but the patient had Fever with Brugada -- A young F is hyperthermic, delirious, and dry: Fever-induced Brugada? Clinical History 2.a. syncope of unclear etiology: +1 2.c.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. What was the outcome and final diagnosis?
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. Pain was resolving. Diagnosed as Normal by the computer. Troponin negative.
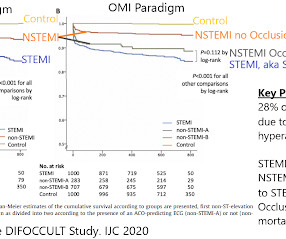
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. And you can see why: the artery may sponstaneously reperfuse, as it did here well before angiography, and documented with resolution of pain and evolution of the ECG to typical full reperfusion pattern Peak troponin I was 8544 ng/L. What did I say?
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 Next trop in AM. Peak trop 257.97 Smith: This is an enormous myocardial infarction. ng/mL - 80.0
Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. ng/mL (ref. < < 0.049).
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He was started on nitro gtt.
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The following ECG was obtained. ECG 1 What do you think?
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Repeat ECG: New developing Q waves in V2 and V3, further confirming evolving OMI.
Gender, race, ethnicity, and socioeconomic disparities are well-documented within the healthcare system. While stroke assessment is documented 38% of the time for patients overall, it is only documented 32% of the time for Hispanic/Latino patients. However, in reality, that’s not always the case.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
He now is his agency's "Clinical Improvement Analyst for STEMI performance and quality assurance.” Of the 23 Occlusion MI patients correctly identified by precordial swirl sign, 19 (83 %) had LAD culprit lesions, and 16 (70 %) were missed by STEMI criteria." This was contributed by a great paramedic, Drew Williams. Literature 1.
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic.
Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. This is the longest lasting I have ever documented a hyperacute T wave without going "up" or "down." Interventionalist at the Receiving Hospital: "No STEMI, no cath. Here is one case of a patient I saw.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician interpretation: "No STEMI."
Figure 1: EKG for Dextrocardia showing STEMI. The second EKG was concerning for STEMI in the precordial leads (see figure 1). This delay in recognition can result in the inadvertent underdiagnosis of STEMIs. Dextrocardia with STEMI is a rare clinical presentation that presents with both diagnostic and technical challenges.
Appropriate air medical services utilization and recommendations for integration of air medical services resources into the EMS system of care: a joint position statement and resource document of NAEMSP, ACEP, and AMPA. Air medical transport has been utilized in multiple hospital based programs including trauma, STEMI, and stroke.
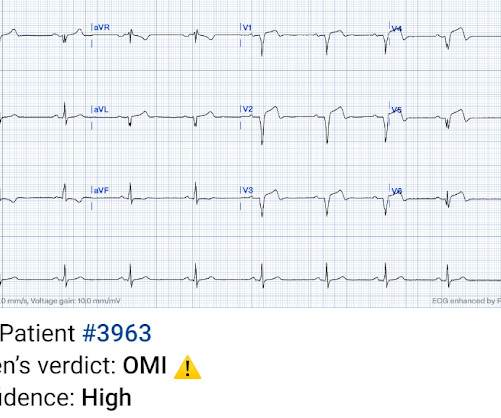
This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria. This was sent to me by a friend.
This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. But it does not meet STEMI criteria and it was not initially recognized. ng/mL (very elevated).
The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. To me, that is a meaningless diagnosis. Here is the main learning point: The infarct was due to an occluded artery (Occlusion MI, OMI). In 30% of OMI, there is no significant ST Elevation.
After admission he undergoes another ECG, though it is unclear from documentation whether there was a change in his chest pain. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
Meyers note: notice in their documentation many of the classic mistakes of the STEMI generation: "Non ST Elevation MI" as their reasoning for why the patient did not merit emergent reperfusion, while simultaneously calling it "emergently" (after 8 hours!!!) Because we are hypnotized the STEMI paradigm. "If
See many examples of Pseudo STEMI due to hyperkalemia at these two posts: Acute respiratory distress: Correct interpretation of the initial and serial ECG findings, with aggressive management, might have saved his life. And, there is no documentation that the tachycardia has resolved. The patient was treated.
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. This difficulty results in high lateral OMI being the most commonly missed OMIs by the misguided STEMI criteria.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. But which myocardial walls are affected?
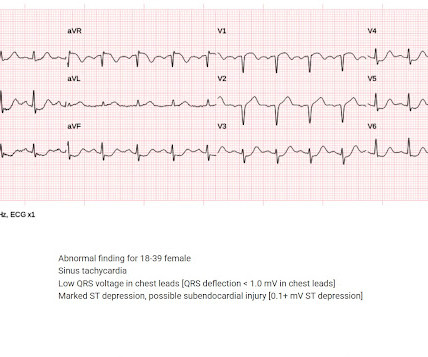
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Learning Points: This is one of many examples of false positive STEMI criteria, which is distinguishable by expert humans, and now by AI such as QOH. No prior ECG was available.
I’ve attached an article and an abstract (that article is in Japanese unfortunately … ) that do document that you CAN however on occasion find AIVR in otherwise healthy children — and I suppose that IS what we have here. Is there STEMI? AIVR is NOT common in otherwise healthy children. Most physicians, at first glance, get this wrong.
T his is a systematic failure that has been documented in the following study: Garg A, Lehmann MH. OMI often does not meet STEMI criteria. If you rely on STEMI criteria, or on the computer algorithm, many of your patients will progress to a completed MI. Circ Arrhythm Electrophysiol. 2013;6(1):76-83.
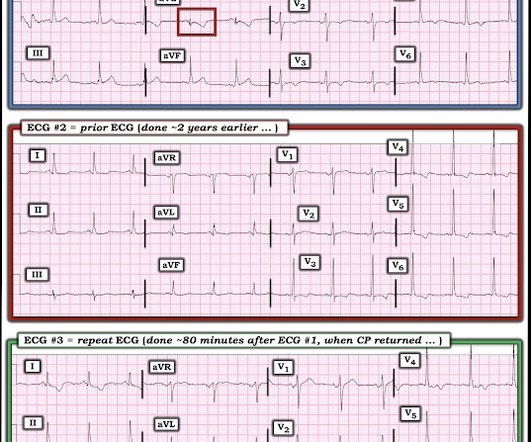
The triage ECG was interpreted correctly as "No STEMI." This finally prompted a repeat ECG at 1341: 1350: Obviously STEMI(+) OMI. Compared to baseline, there is more STE in anterior leads, and significantly increased area under the curve of the T wave in V3 and V4. The second troponin returned higher at 45 ng/L.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content